CDC Reports Initial Cases of HIV/AIDS in Los Angeles
U.S. Centers for Disease Control and Prevention reports cases of a rare lung infection in five young, previously healthy, gay men in Los Angeles — the first official reporting of what would become known as the AIDS epidemic. Two of the men have already died.
Learn More.
The CDC’s Morbidity and Mortality Weekly Report described the men as having additional infections, indicating that their immune systems were compromised. By the time the report was published, two of the young men were already dead.
While this was the first official reporting of the disease, the history of the AIDS epidemic actually reaches back to the early 20th Century, when Simian Immunodeficiency Virus made the jump from chimpanzees to humans in Central Africa.
The new virus began infecting residents in Léopoldville (now Kinshasa) in the Democratic Republic of the Congo some time between 1990 and 1920. according to History.com/A&E Networks. More than 60 years later, when HIV tests became available, blood samples from a Congolese man who died in 1959 tested positive for HIV and this was the first confirmed HIV-related death.
But the existence and spread of HIV had gone unreported in the medical community until around 1980, when a handful of doctors serving urban populations in the U.S. started to see unusual symptoms in their patients.
One of these doctors was Michael Gottlieb, a young immunologist at UCLA (University of California Los Angeles) who diagnosed a rare lung infection in five young men between 1980-1981. Dr. Gottlieb arranged for his findings to be disclosed to the medical community in the CDC’s weekly alert, MMWR.
Dr. Gottlieb encountered his first patient with unusual infections in November 1980, when one of his medical school residents reported a young patient suffering from a severe yeast infection in his throat. When the patient began having breathing difficulties, Dr. Gottlieb arranged to receive a scraping of the patient’s lung tissue through a non-surgical procedure. He was astounded by the test results.
The patient tested positive for Pneumocystis carinii pneumonia (PCP), a rare lung infection, in addition to oral candidiasis, also known as thrush. Dr. Gottlieb then reached out to a colleague who specialized in the new science of T-cells, the white blood cells important to the immune system. The colleague tested the patient’s blood and found that the sample had no T-helper cells, a result so astounding that he ran the test again, with the same results.
In February 1981, Dr. Gottlieb would come across another young man suffering with PCP and depleted T-cells, and shortly after that, a third patient was referred to him. Thorough examinations of the patients about their lifestyles yielded the information that were gay, but Dr. Gottlieb couldn’t determine how their sexual identity was relevant.
A fourth PCP patient appeared in April 1981, and then a report of a fifth man who already died (an autopsy found PCP). Seeing an alarming trend, Dr. Gottlieb contacted an editor at the New England Journal of Medicine, the most prestigious medical journal in the U.S., and was told that the submission-review-publication process would take at least four months. He believed this information needed to get out to the medical community fast, so he instead submitted his report to the CDC’s weekly newsletter, the Morbidity and Mortality Weekly Report(MMWR), a weekly report read by medical officials concerned with infectious disease and public health.
Assisting Dr. Gottlieb in publishing his report was Dr. Wayne Shandera, who worked in the Los Angeles County Department of Public Health as a CDC liaison.
“Gottlieb talked through the charts while Shandera put the information into the dry, turgid prose that the MMWR preferred,” wrote Randy Shilts in his epic recounting of the early years of the AIDS pandemic, And the Band Played On: Politics, People, and the AIDS Epidemic. “The report noted the links between PCP, CMV (cytomegalovirus), and the oral candidiasis that commonly preceded the pneumonia.”
Dr. Gottlieb’s report also stated, “The fact that these patients were all homosexuals suggests an association between some aspect of homosexual lifestyle or disease acquired through sexual contact and Pneumocystis pneumonia in this population.”
The five Los Angeles men in Dr. Gottlieb’s report were not the only early cases in the U.S. Starting around 1979, previously healthy men in New York City and San Francisco were their seeing doctors and baffling them with a range of symptoms that included fatigue, enlarged lymph nodes, flat purple lesions, oral candidiasis, shortness of breath, eczema, fevers, and amebic dysentery. Their medical charts would be marked with notes like “fever of unknown origin,” “Kaposi’s sarcoma,” “cytomegalovirus,” and “toxoplasmosis.” But the traditional treatments for these conditions were not working.
While sporadic cases of AIDS were documented prior to 1970, available data suggests that the epidemic started in the mid- to late 1970s. Grethe Rask, a Danish physician who worked in the Congo, died of pneumonia on December 12, 1977 after suffering for several years from opportunistic infections. Ten years after her death, samples of her blood were tested and found to be positive for HIV.
By 1980, HIV may have already spread to five continents (North America, South America, Europe, Africa and Australia), and in this period, it is possible that up to 300,000 people were already infected.
In April of 1980, the CDC received a report on Ken Horne, a gay man in San Francisco who was diagnosed with Kaposi’s sarcoma. Horne died on November 30, 1981. The CDC would retroactively identify Horne as the first American patient of the AIDS epidemic.
Following Dr. Gottlieb’s report in the CDC’s MMWR, he and his team published a more detailed report in the New England Journal of Medicine on December 10, 1981.
Today, Dr. Gottlieb is an Associate Clinical Professor of Medicine at UCLA’s David Geffen School of Medicine and still treats patients exclusively at AIDS Project Los Angeles (APLA Health). He is also a member of the Council of Advisors to STORIES: The AIDS Monument.
The New England Journal of Medicine, “Pneumocystis carinii Pneumonia and Musocal Candidiasis in Previously Healthy Homosexual Men — Evidence of a New Acquired Cellular Immunodeficiency” by Michael S. Gottlieb, M.D., Robert Schroff, Ph.D., Howard M. Schanker, M.D., Joel D. Weisman, D.O., Peng Thim Fan, M.D., Robert A. Wolf, M.D., and Andrew Saxon, M.D.; December 10, 1981
June 1981
Rare Kaposi’s Sarcoma Found among Gay Men in NY & CA
New York City dermatologist Dr. Alvin Friedman-Kien calls the CDC to report a cluster of cases of a rare and unusually aggressive cancer among gay men in New York and California.
Learn More.
Dr. Friedman-Kien, whose clientele were primarily young men who identified as gay, said he was surprised at the finding that previously healthy men were developing Kaposi’s Sarcoma (KS), a rare cancer historically associated with elderly men of Eastern European or Mediterranean descent.
KS is also associated with people who have weakened immune systems, according to the U.S. National Institutes of Heath (NIH). The disease often presents as a purple plaque on the skin or internal surface of the mouth. KS can also manifest on internal organs, such as the lungs and gastrointestinal system.
Dr. Friedman-Kien told New York magazine:
“In February 1981, I saw a young man who was perfectly healthy except for a number of spots on his skin. I’d never seen anything like it, so I did a biopsy. Under the microscope, the cell structure was clear: it was Kaposi’s sarcoma.”
Dr. Friedman-Kien continued: “A week later, another physician sent me another patient, also a gay man in his late thirties, also with disseminated KS.”
Later research would establish that AIDS-related KS is the second most common tumor in HIV patients with CD4 counts less than 200 cells, according to the NIH. Up to 30% of HIV patients not taking high-activity antiretroviral therapy (HAART) will develop Kaposi sarcoma.
* * * * * Source:
New York magazine, “Fighting AIDS” by Janice Hopkins Tanne, January 12, 1987
POZ magaine, “A Look Back at the Year a Rare Cancer Was First Seen in Gay Men” by Joseph Sonnabend, M.D., July 13, 2020
The New York Times, “Rare Cancer Seen in 41 Homosexuals” by Lawrence K. Altman, July 3, 1981
June 8, 1981
CDC Report Receives Nationwide Media Attention
News media begin to report out on the MMWR article, and within days, the CDC receives reports from around the country of similar cases of opportunistic infections among gay men.
Learn More.
These news stories — which were published by the Los Angeles Times, San Francisco Chronicle and Associated Press — captured the attention of the gay community and medical personnel nationwide.
In response to the outpouring of reports and concerns to the CDC, the Task Force on Kaposi’s Sarcoma and Opportunistic Infections was created to identify risk factors and to develop a case definition for the as-yet-unnamed syndrome. The Task Force worked under the CDC’s Field Services Division in the Epidemiology Program.
To coordinate the task force, the CDC selected James W. Curran, M.D., who would dedicate much of his life to HIV/AIDS research and would publish numerous research papers on the disease.
Task force members included David M. Auerbach, M.D.; John V. Bennett, M.D.; Philip S. Brachman, M.D.; Glyn C. Caldwell, M.D.; Salvatore J. Crispi; William W. Darrow, Ph.D.; Henry Falk, M.D.; David S. Gordon, M.D.; Mary E. Guinan, M.D.; Harry W. Haverkos, M.D.; Clark W. Heath, Jr., M.D.; Roy T. Ing, M.D.; Harold W. Jaffe, M.D.; Bonnie Mallory Jones; Dennis D. Juranek, D.V.M.; Alexander Kelter, M.D.; J. Michael Lane, M.D.; Dale N. Lawrence, M.D.; Richard Ludlow; Cornelia R. McGrath; James M. Monroe; David M. Morens, M.D.; John P. Orkwis; Martha F. Rogers, M.D.; Wilmon R. Rushing; Richard W. Sattin, M.D.; Mary Ellen Shapiro; Thomas J. Spira, M.D.; John A. Stewart, M.D.; Pauline A. Thomas, M.D.; and Hilda Westmoreland.
In its first year, the Task Force on Kaposi’s Sarcoma and Opportunistic Infections received case reports from the following doctors working in New York, San Francisco and Los Angeles:
Donald F. Austin, M.D.; Erwin Braff, M.D.; James W. Buehler, M.D.; James Chin, M.D.; J. Lyle Conrad, M.D.; Selma Dritz, M.D.; Diane M. Dwyer, M.D.; Shirley L. Fannin, M.D.; Yehudi M. Felman, M.D.; Stephen M. Friedman, M.D.; Robert A. Gunn, M.D.; John P. Hanrahan, M.D.; Robert J. Kingon, M.D.; Michael D. Malison, M.D.; Stanley I. Music, M.D.; Mark A. Roberts, M.D.; Alain J. Roisin, M.D.; Richard B. Rothenberg, M.D.; and R. Keith Sikes, M.D.
Frontline | PBS, “Interview: Jim Curran,” interviews conducted Jan. 18, 2005 and Feb. 15, 2006
The New England Journal of Medicine, “Epidemiologic Aspects of the Current Outbreak of Kaposi’s Sarcoma and Opportunistic Infections,” January 28, 1982
June 16, 1981
First Person with AIDS Admitted to NIH
A man exhibiting symptoms of severe immunodeficiency is the first person with AIDS to be admitted to the Clinical Center at the National Institutes of Health.
Learn More.
The 35-year-old, white gay man from New York City was transferred from a Connecticut hospital to the NIH in Bethesda, Maryland after researchers at the National Cancer Institute, an NIH branch that studied immunodeficiency diseases, heard about his case.
Almost immediately after the new disease emerged on the medical scene, researchers recognized that patients with this unnamed syndrome often developed a rare cancer called Kaposi’s sarcoma as well as other tumors, such as high-grade B-cell lymphomas. As a result, some of the earliest AIDS patient care and research was performed by cancer specialists at the NIH and elsewhere.
The man admitted to the NIH was, for privacy purposes, referred to as “Patient D.” He came to the NIH from Hartford Hospital, where he had been hospitalized for two months with neumocystis carinii pneumonia, lymphocytopenia, cytomegalovirus, herpes simplex II, Candida esophagitis, and Mycobacterium avium tuberculosis of the lung, bone marrow, and esophagus.
The patient had been healthy through adulthood until February 1981, when he began experiencing fatigue and weakness, followed by weight loss and fever.
Thomas A. Waldmann, M.D., one of the NIH doctors who was first to examine “Patient D” said in a 1990 NIH interview:
“The pattern that we observed in our patient was the kind of pattern one saw in Hodgkin’s disease patients who were profoundly anergic [i.e., a condition in which the body fails to react to an antigen], or in patients with a form of profound immunodeficiency called ‘severe combined immunodeficiency of infancy,’ where the patient cannot make an effective cellular or antibody immune response. What we were seeing was an acquired form of cell-mediated immunity.”
Dr. Waldmann said the medical team performed every test they could think of to try to determine the cause of Patient D’s condition, to no avail.
“We were all groping, trying to understand what was going on,” Dr. Waldmann recalled. “In that era, one couldn’t be fatalistic, even when someone was in an apparently irreversible state. One had to assume that somehow one might be able to reverse the immunodeficiency and with that bring into control the infectious disease.”
Members of the NIH’s Metabolism Branch joined forces to study the patient’s cells in a variety of tests. Once doctors determined that Patient D suffered from a rare case of cytomegalovirus retinitis, the National Eye Institute became involved, photographing and studying Patient D’s deteriorating eyesight.
In addition to the research, the doctors were scrambling to find a treatment that Patient D would respond to, but these treatments failed to reverse the course of the symptoms. In fact, it would later be discovered that chemotherapy, the traditional treatment for many forms of cancer, would be ineffective for (and even harmful to) AIDS patients because of their weakened immune systems.
“At the end, the patient had massive cerebral necrosis and autolysis. We had a great number of people involved in treating all the different systems,” Dr. Waldmann said in 1990. “His disease continued, and the patient finally died on October 28, 1981 of hypotension and respiratory failure, with multisystem involvement.”
An autopsy of the body revealed an even wider spectrum of infectious diseases, including massive necrosis, encephalitis, and degeneration of the brain.
AIDS researcher and early human immunodeficiency virus (HIV) drug developer Robert Yarchoan, M.D., recalled the gravity of the moment:
“AIDS showed us that something that no one ever worried about before suddenly could become a major problem for the country and for mankind. And when HIV was identified as the cause of AIDS, it became apparent that, in addition to persons known to have AIDS, thousands of people in the United States were already infected with this new virus without knowing it. Moreover, at this time, infection with HIV was in most cases fatal.”
National Institutes of Health, “Dr Thomas Waldmann Oral History 1990,” interview of Dr. Waldmann on March 14, 1990 by interviewers Dennis Rodrigues, Program Analyst, and Dr. Victoria Harden, Director of the NIH Historical Office.
June 30, 1981
UCSF Researchers Identify Oral Lesion as AIDS Precursor
The husband-and-wife academic team of John and Deborah Greenspan are first to identify hairy leukoplakia, an oral lesion which is a precursor to HIV and AIDS, while conducting research at the University of California San Francisco’s School of Dentistry.
Learn More.
When Dr. Deborah Greenspan started seeing a white lesion on the tongue of gay men coming to her clinical practice, she consulted with her pathologist husband, who suggested a biopsy to find out what was causing it. Dr. John Greenspan (1937-2023) identified the oral lesions as a rare form of cancer which impacted the lymphatoid system, and he decided it warranted a closer look.
“I thought this was strange,” he said in 2012 on the occasion of receiving the Gold Medal Award for Excellence in Dental Research. “We typically saw it in Africa. But in this country, we only used to see it rarely — for example, in immunosuppressed patients, such as kidney transplant recipients. So, we ended up seeing one of the first AIDS lymphoma patients reported in the world.”
The Greenspans conducted studies that showed the lesions — dubbed “oral hairy leukoplakia” (HL) because of its corrugated or shaggy appearance — failed to respond effectively to the usual treatment of antifungal applications. In fact, many of their patients already had or soon developed other immune-depressed symptoms associated with AIDS, such as pneumocystis carinii pneumonia (PCP) and Kaposi’s sarcoma (KS).
The Greenspans would then go on to establish a connection between HL and Epstein-Barr virus (EBV) in a 1985 report. By 1987, they would be able to announce that HL and EBV were symptoms associated with AIDS.
They would continue their work at UCSF over the next 30-plus years, leading a series of studies relating to the mouth and HIV/AIDS. Their work has been instrumental in teaching physicians, nurse practitioners and other clinicians how to identify oral lesions associated with HIV infection.
“The work of Dr. Greenspan and his colleagues has provided guidelines that enable dentists to recognize early oral manifestations of HIV/AIDS and thereby assist with early diagnosis and referral for treatment,” said John Featherstone, dean of the UCSF School of Dentistry. “This is of particular importance in the global health world.”
July 1, 1981
Doctors Identify More Cases in San Francisco & New York City
As his first day as an oncologist at San Francisco General Hospital, Dr. Paul Volberding treats his first HIV-positive patient, a 22-year-old man with Kaposi sarcoma (KS). The man would die a short time later.
Learn More.
After completing a three-year fellowship at the University of California San Francisco, Dr. Volberding was ready to become a cancer specialist under renowned virologist Dr. Jay Levy. Instead, he found himself on a lifelong journey of treating people living with HIV/AIDS and fighting the spread of the virus.
“Twenty-two-year-old man, grew up in the Deep South, and as I recall he was estranged from his family,” Dr. Volberding told the San Francisco Examiner almost 35 years later. “He ended up in San Francisco working basically sex for food, and had innumerable previous sexually transmitted infections.”
The man died within a few months, without his family present, Dr. Volberding recalls.
Around this same time in the early summer of 1981, two doctors in the Bronx started to see HIV/AIDS symptoms in their own patients. Dr. Gerald Friedland identified several cases of Pneumocystis pneumonia in injection drug users, and became one of the first to see the connection between IV-drug use and HIV transmission.
Pediatric immunologist Dr. Arye Rubenstein began to identify the immunodeficiency of his pediatric patients, the children of drug addicts, as a symptom of what would be eventually called AIDS.
Dr. Rubenstein, who had been seeing this particular kind of immunodeficiency in children and sometimes in their mothers in his Bronx practice since the late 1970s, was one of the first to connect pediatric cases to the new disease affecting homosexual men.
These doctors who treated some of the first known cases of HIV/AIDS went on to do important, transformative work in the fields of treatment, research and public health policy.
In 1983, Dr. Volberding established what would make San Francisco General Hospital the model for HIV care: the country’s first AIDS treatment center (Ward 86). Later the same year, he joined the medical team at Ward 5B, the world’s first in-patient clinic for AIDS patients.
Dr. Volberding continued to treat HIV/AIDS patients until 2012, when he became director of the UCSF AIDS Research Institute. Volberding would also become co-director of the Center for AIDS Research.
In the years to come, Dr. Friedland also dedicated his life to AIDS treatment and research. Following 10 years of working with HIV/AIDS patients in the Bronx, Dr. Friedland became director of the HIV/AIDS Program at Yale and Professor of Medicine and Epidemiology and Public Health at Yale School of Medicine.
Dr. Friedland also became involved in HIV/AIDS international research aimed at providing access to antiretroviral therapy in developing regions of the world. The major focus of his work became the integration of HIV and TB care and treatment in co-infected patients in South Africa.
In 2018, on the occasion of delivering the keynote address at the 13th annual International Conference on HIV Treatment and Prevention, Dr. Friedland told The Body PRO:
“Many of these people living with HIV, I have cared for, for decades. I know them extremely well. They know me. We have gone through this together and have this close collegial relationship as a partnership, so it’s a wondrous pleasure to continue to provide.”
The other doctor working in New York City in 1981, Dr. Rubenstein, would decide to remain in the Bronx, caring for children with HIV AIDS. In 1983, he received a grant from the National Institutes for Health to study the incidence of AIDS in women and children. In 1986, Dr. Rubenstein established that transmission of AIDS can occur in utero, and his breakthrough findings were published in the journal Clinical Immunology and Immunopathology.
By this time, Dr. Rubsenstein had treated more than a hundred HIV-infected children, and in the summer of 1985, he opened a day care center for pediatric AIDS patients at Albert Einstein College of Medicine in the Bronx. He became Chief of the Division of Allergy & Immunology at Children’s Hospital at Montefiore, and Professor of Pediatrics, Microbiology & Immunology at Albert Einstein College.
“Many come from a low socioeconomic group, they’re poor, the family may have broken up, they may have used drugs, and now their child has AIDS because they gave it to him. You wouldn’t be surprised if they threw up their hands, but many don’t. They become the best parents in the world. They straighten out their lives, they spend hours with their kids. They give up longing for material things and look for spiritual and religious values.”
* * * * * Sources:
San Francisco Examiner, “Pioneering AIDS Doctor Reflects on First Cases in SF as City Strives to Eradicate Virus,” February 8, 2015
The Body Pro, “HIV ‘Providers’ Aren’t Just Doctors: An Interview with Gerald Friedland, MD” by Stephen Hicks, June 19, 2018
The New York Times, ” Ideas & Trends: The Strain of Caring for the Littlest AIDS Victims” by Jane Gross, August 4, 1985
July 2, 1981
Mention of ‘Gay Men’s Pneumonia’ Appears in Media
The first mention of “Gay Men’s Pneumonia” is published in the Bay Area Reporter, a weekly newspaper for the gay and lesbian community in San Francisco.
Learn More.
The short item advised gay men experiencing progressive shortness of breath to see their physicians.
* * * * * Source:
Bay Area Reporter, “Health Shorts: ‘Gay Men’s’ Pneumonia,” July 2, 1981
July 1981
CDC Creates Task Force on Kaposi’s Sarcoma & Opportunistic Infections
A Task Force on Kaposi’s Sarcoma and Opportunistic Infections is established at the Centers for Disease Control and Prevention under the direction of Dr. James Curran.
Learn More.
Shortly after MMWR description of five cases of Pneumocystis carinii pneumonia (PCP) among homosexual men in Los Angeles, additional cases of other life-threatening opportunistic infections and a malignancy, Kaposi sarcoma (KS), were reported to the CDC.
Upon learning of these first cases, the CDC formed the Task Force on Kaposi’s Sarcoma and Opportunistic Infections to begin surveillance and conduct epidemiologic investigations. Despite budget constraints at the time, about 30 CDC officers and staff were assigned to the Task Force during the summer of 1981. CDC Director William Foege, appointed epidemiologist James Curran to lead the task force.
The Task Force first worked to establish a case definition for surveillance and investigation of the outbreak. Previously, KS was known as an infrequently-diagnosed cancer that was rarely life-threatening, typically occurring among elderly men. The outbreak seemed to represent a new epidemiologic form of KS.
Between June 1, 1981, and May 28, 1982, CDC would receive 355 case reports of KS and/or serious opportunistic infections, especially Pneumocystis carinii pneumonia, occurring in previously healthy persons between 15 and 60 years of age. Of the 355, 281 (79%) were homosexual (or bisexual) men, 41 (12%) were heterosexual men, 20 (6%) were men of unknown sexual orientation, and 13 (4%) were heterosexual women.
Five states — California, Florida, New Jersey, New York, and Texas — accounted for 86% of the reported cases.
Morbidity and Mortality Weekly Report | Centers for Disease Control and Prevention, “Epidemiologic Notes and Reports Update on Kaposi’s Sarcoma and Opportunistic Infections in Previously Health Persons — United States,” June 11, 1982
August 28, 1981
CDC Reports that 40% of Identified Cases Die of KS/PCP
Of the 108 known cases of Kaposi’s Sarcoma and pneumocystis carinii pneumonia, 107 are male and 94% of those whose sexual orientation is known are gay/bisexual. About 40% of all patients have already died.
News of the article alarms the gay community for its indication that the new disease is spreading and that the outcome of those infected was likely to be a quick and brutal death.
Small Medical Conference is First to Address Epidemic
Fifty leading clinicians gather in Bethesda, Maryland for the first conference to address the new epidemic.
Learn More.
Cosponsored by the National Cancer Institute and Centers for Disease Control and Prevention, the medical conference focused on Kaposi’s sarcoma and other opportunistic infections. Researchers began to develop recommendations for further studies in epidemiology, virology, and treatment.
National Institutes of Health, “In Their Own Words: NIH Researchers Recall the Early Years of AIDS | Timeline (1981-1988)”
September 21, 1981
First AIDS Clinic Opens in San Francisco
The Kaposi’s Sarcoma clinic at the University of California’s San Francisco Medical Center opens its doors, becoming the first clinic in the world to exclusively treat what would become to be known as AIDS.
Dr. Conant would go on to create the San Francisco AIDS Foundation (first called the Kaposi’s Sarcoma Research and Education Foundation) to address both the need to go into the community, which was still in denial about the disease, and the need to find non-government funding sources.
On July 1, 1981, Dr. Volberding saw his first patient with Kaposi’s sarcoma (KS), a rare cancer later linked to AIDS, on his first day working at San Francisco General Hospital.
The New York Times, “Constance Wofsy, 53, Doctor Who Directed an AIDS Program,” June 9, 1996
San Francisco Chronicle, “The Good Doctor: He’s been in on the AIDS Battle Since the Beginning,” August 12, 2001
December 1981
Pediatric AIDS Cases Surface in New York City
At Albert Einstein Medical College in New York, pediatric immunologist Dr. Arye Rubinstein treats five Black infants showing signs of severe immune deficiency, including pnuemocytis carinii pneumonia.
Learn More.
The mothers of at least three of the children disclosed that they used drugs and/or engaged in sex work. Dr. Rubinstein recognized that the children were showing signs of the same illnesses affecting gay men, but his diagnoses were initially dismissed by his colleagues.
“This would ultimately prove to be the moment when AIDS emerged in the Black community, driven among men, women, and children by sexual contacts, injecting drug use, and mother-to-child transmission,” writes Michael Broder in his article for Positively Aware.
By 1987, pediatric AIDS cases would be on the rise, especially in New York and especially among minority groups. Many babies would be orphaned, creating insurmountable challenges for social workers seeking foster care placements for them.
Although medical experts estimated the number of infected infants in the city to be as many as 3,000, the City of New York has only 241 recorded cases of pediatric AIDS by the end of 1987. Of these cases, the racial breakdown was 59% Black, 32% Hispanic and 8% White.
The New York Times, “For Child With AIDS, Hospital Is Home” by Bruce Lambert, December 24, 1987
December 5, 1981
Pamphlet on KS Distributed to Conference Attendees
In an attempt to alert the medical community to the yet-unnamed disease afflicting young gay men, three dermatologists from San Francisco and New York City distribute a pamphlet on Kaposi’s sarcoma to attendees of a dermatology conference.
Learn More.
Drs. Marc Conant, Alvin Friedman-Kien, and James Groundwater stationed themselves at the entrance of the annual meeting of the American Academy of Dermatology and distributed to incoming attendees a pamphlet they hastily put together about Kaposi’s sarcoma, a rare form of skin cancer that was being diagnosed in previously healthy young men in San Francisco and New York City.
Held on Dec. 5-10, the conference drew thousands of dermatologists in the United States and Canada to San Francisco to hear the latest developments in their medical field. The pamphlet was likely the first information that most conference attendees received about Kaposi’s sarcoma (KS) and its role in the yet-unnamed disease of AIDS.
“At that point in time, not many people knew about this problem, and it wasn’t getting a whole lot of attention,” Dr. Groundwater later recalled for the San Francisco AIDS Oral History Project. “I don’t think the seriousness of it was widely appreciated — the potential for major problems in the future.”
Dr. Groundwater said he wrote the copy for the brochure and used photographs of a patient’s KS lesions so dermatologists could see how the disease manifested. The patient was Ken Horne, the first KS case to be reported to the Centers for Disease Control. Horne had died on November 30, 1981, just days before the conference.
* * * * * Source:
University of California Libraries, “The San Francisco AIDS Oral History Series | The AIDS Epidemic in San Francisco: The Response of Community Physicians, 1981-1984,” interview with James R. Groundwater, M.D., conducted by Sally Smith Hughes, Ph.D. in 1996
December 31, 1981
45% of Patients Die by Year-End
At the close of 1981, a cumulative total of 270 cases of severe immune deficiency are reported among gay men, and 121 of those individuals have died.
Learn More.
By this time, some researchers began to call the condition GRID (Gay-Related Immune Deficiency). This terminology would have a negative influence on both the medical profession and the public, causing people to perceive the epidemic as limited to gay men.
This early misconception of the disease would have serious long-term consequences as it becomes evident that anyone could be infected with HIV, including women, heterosexual men, hemophiliacs, people who inject drugs, and children.
U.S. Public Health Service Hosts AIDS Conference at CDC
U.S. Public Health Service hosts a conference on AIDS at the Centers for Disease Control and Prevention in Atlanta.
Learn More.
At the conference, researchers debate whether the opportunistic infections were being caused by one or more transmissible or immune-suppressing agents.
The New York Times publishes the first media mention of the term “GRID” (Gay-Related Immune Deficiency), deepening public perceptions that HIV/AIDS is solely related to homosexuality.
Learn More.
Under the headline “New Homosexual Disorder Worries Health Officials,” the Times introduced its readers to “a serious disorder of the immune system” that had proved fatal in 136 people to date.
“It was colloquially referred to as GRID – ‘Gay Related Immune Deficiency’ or ‘Gay Related Immune Disease,’ as if there was something intrinsic about being gay that made people susceptible to it,” wrote Carla Tsampiras in The Conversation.
While the Times article identified 13 cases of the disease in heterosexual women, it went on to state, “Most cases have occurred among homosexual men, in particular those who have had numerous sexual partners, often anonymous partners whose identity remains unknown.”
Even once the disease was renamed HIV/AIDS, the stigmatization continued. Early research elicited categories of people, referred to as “high-risk groups,” who were apparently at increased risk of having AIDS. They were informally known as “the Four-H Club” — homosexuals, Haitians, hemophiliacs and heroin users. Later, “hookers” were added to the list.
“As a result, AIDS avatars — such as The Homosexual, The Prostitute, and The Drug Abuser — were created, drawing on long histories of social and medical prejudice and othering of certain groups of people,” said Carla Tsampiras, Senior Lecturer in Medical Humanities at the University of Cape Town. “The avatars drew on existing stereotypes and reinforced them, reflecting existing prejudices or social attitudes relating to sexuality, sexual orientation, race, class and gender.”
* * * * * * Sources:
The New York Times, “New Homosexual Disorder Worries Health Officials” by Lawrence K. Altman, May 11, 1982
The Conversation, “AIDS: What Drove Three Decades of Acronyms and Avatars?” by Carla Tsampiras, June 4, 2015
June 18, 1982
Researchers Connect AIDS Transmission to Sex
The Centers for Disease Control publishes an MMWR article that is the first to suggest sexual transmission as the source of Karposi’s sarcoma and other opportunitic infections in gay men.
Learn More.
The MMWR article describes a potential sexually transmitted agent as being the link to outbreaks of KS, Pneumocystis carinii pneumonia (PCP), and other infections recently found among young gay men.
The report describes a study of 19 case subjects from June 1, 1981 to April 12, 1982 involving biopsy-confirmed KS and/or PCP among previously healthy male residents of southern California. Following a report of possible personal connections among the KS/PCP case subjects in Los Angeles and Orange counties, interviews were conducted with the eight subjects still living and with seven of the close friends of 11 subjects who had died.
Through these interviews, the CDC was able to collect data on sexual partners for 13 of the 19 subjects. The study considered “sexual contact” to be established if the KS/PCP case subjects was reported to have “exposure” to another person that was either substantiated or not denied by the other person involved in the relationship (or by a close friend of that person).
Within five years of the onset of symptoms, nine of the KS/PCP case subjects had had sexual contact with others who had KS or PCP. They consisisted of seven case subjects from LA County who had sexual contact with other patients from LA County, and two case subjects from Orange County had sexual contact with one patient with KS who resided outside California.
Four of the nine KS/PCP case subjects had been exposed to more than one patient who had KS or PCP. Three of the nine KS case subjects developed their symptoms after sexual contact with persons who already had symptoms of KS. One of these three subjects developed symptoms of KS about nine months after sexual contact, another subject developed symptoms 13 months after contact, and a third subject developed symptoms 22 months after contact.
The other four KS/PCP case subjects in the group of 13 had no known sexual contact with reported cases. However, one KS case subject had an apparently healthy sexual partner in common with two persons with PCP; one KS case subject reported having had sexual contact with two friends of the non-Californian with KS; and two PCP case subjects had most of their anonymous contacts (greater than or equal to 80%) with persons in bathhouses.
The editorial note to the report included these points:
An estimated 185,000-415,000 homosexual males lived in LA County in 1982.
If one assumes each homosexual male in LA County has between 13 and 50 different sexual partners per year during 1977-1982, “the probability that seven of 11 patients with KS or PCP would have sexual contact with any one of the other 16 reported patients in LA County would seem to be remote.”
With this same assumption, “the probability that two patients with KS living in different parts of Orange County would have sexual contact with the same non-Californian with KS would appear to be even lower.”
Thus, observations in LA and Orange counties imply the existence of an unexpected cluster of cases.
The CDC then puts forth the hypothesis that infectious agents are being sexually transmitted among homosexually active males.
“Infectious agents not yet identified may cause the acquired cellular immunodeficiency that appears to underlie KS and/or PCP among homosexual males. If infectious agents cause these illnesses, sexual partners of patients may be at increased risk of developing KS and/or PCP,” the CDC report posits.
The CDC proposes another hypothesis: “Sexual contact with patients with KS or PCP does not lead directly to acquired cellular immunodeficiency, but simply indicates a certain style of life. The number of homosexually active males who share this lifestyle may be much smaller than the number of homosexual males in the general population.”
The CDC goes on to suggest the possibility of exposure to “some substance (rather than an infectious agent)” leading to immunodeficiency among homosexual males that share a particular style of life.
The report cites a New York City-based report suggesting a connection between amyl nitrite (commonly referred to as “poppers”) and an increased risk of KS. This hypothesis would later be scientifically disproved.
* * * * * Sources:
Mortality and Morbity Weekly Report, “A Cluster of Kaposi’s Sarcoma and Pneumocystis carinii Pneumonia among Homosexual Male Residents of Los Angeles and range Counties, California,” June 18, 1982
June 27, 1982
Play Fair! First to Advocate for Safe Sex Practices
The Sisters of Perpetual Indulgence creates Play Fair! — the first “safer sex” pamphlet to address the growing AIDS epidemic.
Learn More.
The Sisters distributed 16,000 copies of Play Fair! during the San Francisco Gay & Lesbian parade in June 1982.
Written by Sister Florence Nightmare and Sister Roz Erection, who outside the Order were known as registered nurses Bobbi Campbell and Baruch Golden, Play Fair! was among the first guides promoting safe sex and raising awareness around sexually transmitted diseases.
The Sisters originated in 1979 with three gay men who wanted to combine radical politics, street theater, and high camp, according to Will Kohler. Having obtained nuns’ habits from a community theater production of The Sound of Music, these men (a.k.a., Sister Vicious Power Hungry Bitch, Sister Missionary Position, and Sister Roz Erection ) turned heads as they strolled Castro Street on Easter Sunday.
By 1982, the Sisterhood had many members and promoted a lively campaign around sex-positivity through a combination of fundraising, community outreach and events. With growing anxiety and concern around the spread of Kaposi’s sarcoma and other immune disorders among gay men, it was inevitable that the Sisters would incorporate AIDS awareness into its mission.
Although originally founded as an “Order of Gay Male Nuns,” the group now includes gay, lesbian, bisexual, heterosexual, and transgendered men and women. Many of their rituals are influenced by Eastern religious practices and beliefs, as well as by Roman Catholicism. Their doctrine stresses universal joy and the expiation of guilt.
Members of the Sisters of Perpetual Indulgence who have died are referred by the Sisters as “Nuns of the Above.”
Back2Stonewall, “Gay History – April 15, 1979: San Francisco’s Sisters of Perpetual Indulgence Founded,” April 16, 2022
The Culture Trip, “Meet the Sisters of Perpetual Indulgence, San Francisco’s Order of Queer Nuns” by Deanna Morgado, July 3, 2019
GLBTQ Archive, “Sisters of Perpetual Indulgence” by Robert Kellerman, 2002
July 9, 1982
32 Haitian Immigrants Diagnosed with Opportunistic Infections & KS
The Centers for Disease Control and Prevention reports a “cluster” of opportunistic infections and Kaposi’s sarcoma among Haitians who recently entered the U.S.
Learn More.
In the summer of 1982, life-threatening opportunistic infections and Kaposi’s sarcoma were reported among 32 Haitian migrants to the United States. The CDC stated in its Morbidity and Mortality Weekly Report that most were heterosexual men with no known risk factors who had migrated from Haiti within the past two years.
The MMWR also mentioned that the CDC received reports of KS cases in Port-Au-Prince, and the combined reports indicated “an epidemiologically distinct pattern of illness” that occurred via heterosexual transmission.
Years later, in its report “AIDS: The Early Years and CDC’s Response,” the CDC conceded that by publicly reporting these cases as “Haitian entrants,” the CDC inadvertently contributed to the stigma associated with “AIDS labeling.” This stigma would be endured by thousands of Haitian migrants fleeing poverty and political persecution in the 1980s and 1990s.
From April 1, 1980 through June 20, 1982, 19 Haitian patients were admitted to Jackson Memorial Hospital in Miami with evidence of opportunistic infections (including Pneumocystis carinii pneumonia, cryptococcal meningitis or fungemia, toxoplasmosis, and esophageal candidiasis) and one patient also had Kaposi’s sarcoma. Seventeen were men and two were women. At the time the CDC released its MMWR, 10 of the 19 Haitian immigrants in Florida had already died. Their average age was 28 years old.
From July 1, 1981, through May 31, 1982, 10 Haitian residents of Brooklyn, New York — all men, aged between 22 and 37 years old — were diagnosed with opportunistic infections (including Pneumocystis carinii pneumonia, cryptococcal meningitis or fungemia, toxoplasmosis, and esophageal candidiasis). Five of the 10 immigrants in Brooklyn had already died.
The remaining three cases were reported from health officials in California, Georgia, and New Jersey.
The CDCwarned medical officials and doctors who care for Haitian patients to “be aware that opportunistic infections may occur in this population.”
July 16, 1982
CDC Identifies Hemophilia-AIDS Connection
CDC reports three cases of hemophiliacs diagnosed with pneumocystis carinii pneumonia, a common AIDS-related illness.
Learn More.
The CDC’s MMWR article is the first report of the AIDS-related condition of immunosuppression in patients with hemophilia who have no other known risk factors for AIDS.
By the time the MMWR article is published, two of the three subjects have died.
In a report to the medical community, the Centers for Disease Control and Prevention coins the term “AIDS” — Acquired Immune Deficiency Syndrome.
Learn More.
The MMWR article also includes the first case definition for AIDS: “A disease at least moderately predictive of a defect in cell-mediated immunity, occurring in a person with no known cause for diminished resistance to that disease.”
Today, AIDS is defined as a set of symptoms (or syndrome) caused by the HIV virus. A person is said to have AIDS when their immune system is too weak to fight off infection. This is the last stage of HIV, when the infection is very advanced.
The Centers for Disease Control and Prevention lays out the first set of precautions for clinical and lab staff working with people with AIDS symptoms.
The report noted that “airborne spread and interpersonal spread through casual contact do not seem likely.”
Those providing care to people with AIDS were advised the following:
Extraordinary care must be taken to avoid accidental wounds from sharp instruments contaminated with potentially infectious material and to avoid contact of open skin lesions with material from AIDS patients.
Gloves should be worn when handling blood specimens, blood-soiled items, body fluids, excretions, and secretions, as well as surfaces, materials, and objects exposed to them.
Gowns should be worn when clothing may be soiled with body fluids, blood, secretions, or excretions.
Hands should be washed after removing gowns and gloves and before leaving the rooms of known or suspected AIDS patients. Hands should also be washed thoroughly and immediately if they become contaminated with blood.
Blood and other specimens should be labeled prominently with a special warning, such as “Blood Precautions” or “AIDS Precautions.” If the outside of the specimen container is visibly contaminated with blood, it should be cleaned with a disinfectant (such as a 1:10 dilution of 5.25% sodium hypochlorite (household bleach) with water). All blood specimens should be placed in a second container, such as an impervious bag, for transport. The container or bag should be examined carefully for leaks or cracks.
Blood spills should be cleaned up promptly with a disinfectant solution, such as sodium hypochlorite (see above).
Articles soiled with blood should be placed in an impervious bag prominently labeled “AIDS Precautions” or “Blood Precautions” before being sent for reprocessing or disposal. Alternatively, such contaminated items may be placed in plastic bags of a particular color designated solely for disposal of infectious wastes by the hospital. Disposable items should be incinerated or disposed of in accord with the hospital’s policies for disposal of infectious wastes. Reusable items should be reprocessed in accord with hospital policies for hepatitis B virus-contaminated items. Lensed instruments should be sterilized after use on AIDS patients.
Needles should not be bent after use, but should be promptly placed in a puncture-resistant container used solely for such disposal. Needles should not be reinserted into their original sheaths before being discarded into the container, since this is a common cause of needle injury.
Disposable syringes and needles are preferred. Only needle-locking syringes or one-piece needle-syringe units should be used to aspirate fluids from patients, so that collected fluid can be safely discharged through the needle, if desired. If reusable syringes are employed, they should be decontaminated before reprocessing.
A private room is indicated for patients who are too ill to use good hygiene, such as those with profuse diarrhea, fecal incontinence, or altered behavior secondary to central nervous system infections. Precautions appropriate for particular infections that concurrently occur in AIDS patients should be added to the above, if needed.
* * * * * Source:
Mortality and Morbidity Weekly Report, “Current Trends Acquired Immune Deficiency Syndrome (AIDS): Precautions for Clinical and Laboratory Staffs,” November 4, 1982
November 1982
AIDS Takes Center Stage at Medical Conference in Toronto
AIDS is the big topic at the Canadian Public Health Association’s inaugural National Conference on Sexually Transmitted Diseases in Toronto.
Learn More.
In the 10 months leading up to the conference, the number of known AIDS cases in Canada had grown from one to 14. So the issue of AIDS was on the minds of many health officials and medical practitioners attending conference hosted by the CPHA’s new Sexually Transmitted Diseases division.
At the conference, Dr. Marc Steben told participants that, due to a dearth of information from the medical community, gay men had resorted to passing information about the new disease amongst themselves. Dr. Steben would go on to dedicate much of his career to HIV/AIDS treatment and become co-president of HPV Global Action, based in Montréal.
At the time of the conference, 14 AIDS cases had been reported in Canada and 10 people had already died. Eleven of the cases were reported in Montreal, and one each in Vancouver, Toronto, and Windsor. Medical officials were reviewing four more cases that they expected to be AIDS.
Many of the conference attendees were also aware of the publication in the gay weekly Body Politic of two articles: “Living with Kaposi’s” by Michael Lynch and “The Real Gay Epidemic: Panic and Paranoia” by Bill Lewis.
In the first article, Lynch wrote an extensive profile of gay men living with Kaposi’s Sarcoma in New York City. Lynch expressed his concern with the NYC community’s eager embrace of the medical community and its discourses of pathology.
“Gays are once again allowing the medical profession to define, restrict, pathologize us,” Lynch wrote in the November 1982 edition of Body Politic. “What used to be a psychiatric pathology is now an infectious one … This panic could never have set in so quickly and so deeply if within the hearts of gay men there weren’t already a persistent anti-sexual sense of guilt ready to be tapped.”
In his article, Lynch called for a response to AIDS from people who were exclusively gay. Lynch was an American-born English professor who settled in Toronto. He would die of AIDS-related illness on July 9, 1991.
His article in Body Politic was accompanied by a shorter piece by Bill Lewis which argued against panic and urged readers to look at the disease through a lens of science.
“Until recently, the cause of the collapse of the immune system was baffling, and everything gay men did that straight men didn’t was dragged forth as a possible cause,” Lewis wrote. “Abundant sex, poppers, fisting, drugs, ingestion of too much sperm, staying up too late — all have been put forward as an explanation.”
Lynch said that these things failed to make sense as explanations, because none could explain cases of AIDS among nearly celibate gay men, hemophiliacs or children.
According to This is Public Health: A Canadian History, CPHA’s director of the AIDS Education and Awareness Program, David Walters, described Canada’s initial public health response to HIV as “fragmented confusion.”
Canada was facing an economic recession and inadequate healthcare funding from different branches of government. This, along with a lack of coordination efforts at the local level and a general resistance to anything involving the needs of the gay community, contributed to a reluctance by public health officials to take action in the early years of the epidemic.
According to Walters, “There seemed to be no safe ground in talking about homosexuality, condoms and needles at national or provincial levels. This reluctance resulted in foot-dragging and unclear messages about needed commitment to educational programs.”
January 1, 1983
Ward 86: First Dedicated AIDS Outpatient Clinic Opens
Ward 86, the worlds first dedicted AIDS outpatient clinic, opens at San Francisco General Hospital, a partnership with the University of California San Francisco.
Learn More.
Ward 86 becomes the gold standard for treating patients living with HIV/AIDS.
The clinic attracted staff passionate about treating people with AIDS. Over time, the clinic team developed the San Francisco Model of Care, which focused on treating patients with compassion and respect; providing an array of health and social services in one facility; and collaborating closely with the local health department and community organizations.
Founded by AIDS pioneers Drs. Paul Volberding, Donald Abrams and Constance Wofsy, the clinic would see thousands of patients annually, ranging in age from 18 to 82, in the coming years.
In June 1983, the inpatient HIV unit, 5B, would also open at San Francisco General Hospital.
Bay Area Reporter, “Hospital’s HIV/AIDS Division Marks 25th Anniversary” by Seth Hemmelgarn, November 27, 2008
San Francisco Chronicle, “SF AIDS Ward 86 – 25 Years of Saving Lives” by Elizabeth Fernandez, December 1, 2008
January 4, 1983
CDC Shares Data on AIDS & Hemophilia with Red Cross
The Public Health Service hosts a meeting convened by the CDC and attended by 200 members of the blood services community to address opportunistic infections in hemophiliacs. At the meeting, the Red Cross and other blood supply organizations receive preliminary data on the indication of the AIDS virus within the blood supply.
Learn More.
At the conference, scientists from the CDC recommended that blood banks begin implementing donor screening measures, such as questioning donors about risk behaviors and running blood donations through a series of tests. Faced with daunting data and the same uncertainties, the blood banks and the plasma companies came away from the conference with different plans..
Playing down the extent of the risk, leaders of the blood banks would decide that the CDC’s evidence did not show conclusively that HIV was a blood-borne disease, and they would decline to screen out potentially infected donors. The blood bank physicians questioned the validity of the CDC data, which correlated of anti-HBc to AIDS cases among a cohort of homosexuals who attended an STD clinic.
By contrast, the plasma companies concurred with the CDC that there was a good chance HIV was being transmitted by their products. They moved very quickly to switch the source of their supply and introduced new methods to inactivate viruses in plasma derivatives. However, they also decided to keep older product batches on the market, and commercial plasma ended up infecting more people than did donated blood.
Getting blood or plasma out of one person and safely into another is a complex process. Blood banks, such as the Red Cross, obtain almost all of their supply from voluntary donors. They process and then distribute freely donated blood to hospitals, which they charge for their services.
Every year, about 14 million units of blood are donated in the U.S. The American Red Cross collects about 45% of the total, blood banks about 42%, hospitals 11%, and the small remainder is imported. About 3.6 million people receive transfusions of these products every year.
In the 1970s, blood collection and transfusion had a number of risks associated with it, in particular the prevalence of hepatitis in the supply. In late 1982, when evidence began to show that a new disease might be spreading through blood products, things became more complicated.
The blood bank scientists accepted that HIV/AIDS appeared to be a threat to the blood supply, but found it difficult to measure the risk. U.S. surveillance systems were ill-equipped to identify diseases with a long incubation period such as AIDS.
The CDC publishes its first article that includes women among those diagnosed with AIDS.
Learn More.
“Epidemiologic Notes and Reports Immunodeficiency among Female Sexual Partners of Males with Acquired Immune Deficiency Syndrome (AIDS) — New York” includes the first cases of AIDS in women participating in a research study.
The MMWR article described the cases of two women who were sexual partners of men diagnosed with AIDS.
In one case, a 37-year-old Black woman began losing weight in June 1982 and had developed oral candidiasis and swollen lymph nodes a month later. Tests revealed she had Pneumocystis carinii pneumonia (PCP), as well as lymphopenia and a depletion of T-helper cells. She said she was not an intravenous drug user, but her sexual partner since 1976 had a history of IV drug abuse. The woman’s partner died of AIDS in November 1982.
In the second case included in the report, a 23-year-old Hispanic woman developed swollen lymph nodes in early 1982. Tests showed she had elevated immunoglobulin levels, lymphopenia, decreased T-helper cell numbers, and a depressed T-helper/T-suppressor cell ratio. She had no previous illnesses or therapy associated with immunosuppression. Since the summer of 1981, her only sexual partner was a bisexual male who had developed AIDS-related symptoms in 1981.
* * * * * * Source:
Mortality and Morbidity Weekly Report, “Epidemiologic Notes and Reports Immunodeficiency among Female Sexual Partners of Males with Acquired Immune Deficiency Syndrome (AIDS) — New York,” January 7, 1983
January 26, 1983
Opposing Views in CDC & Red Cross Lead to Blood Screening Delays
Following a meeting hosted by the Centers for Disease Control and Prevention on opportunistic infections in hemophiliacs, an American Red Cross interoffice memo is released that indicates strong opposition to a widespread screening of blood supply products.
Learn More.
An American Red Cross interoffice memo blasts the CDC after its January 4 meeting, stating, “CDC is likely to continue to play up AIDS.”
The memo goes on to say; “It has long been noted that CDC increasingly needs a major epidemic to justify its existence. To the extent the [blood supply] industry sticks together against CDC, it will appear to some segments of the public at least that we have a self interest which is in conflict with the public interest, unless we can clearly demonstrate that CDC is wrong.”
Donor screening issues arose in mid to late 1982, when cases of AIDS in hemophiliacs were first reported, including the first transfusion-associated AIDS case in an infant.
Between December 1982 and December 1983, there were two critical events that presented opportunities for the blood services community to enact new donor screening and deferral policies to reduce the threat of HIV transmission through blood and blood products.
The first, which occured on January 4, 1983, was at the Public Health Service meeting convened by the CDC. This meeting was widely publicized, and over 200 people attended, including representatives of the FDA, NIH, the National Hemophilia Foundation, the National Gay Task Force, blood banks, and the plasma fractionation industry.
This was where the blood services community first received data on the possibility of a transmissible agent within its blood supply. CDC scientists recommended that blood banks implement specific donor screening measures (such as questioning donors about their risk behaviors and running blood donations through a series of tests).
Some participants in the Atlanta meeting and others in key decision-making roles expressed reservations about the validity of the CDC data and indicated that they did not believe the CDC to be a credible source of information regarding AIDS. Following the conference, American Red Cross officials would encourage colleagues to resist recommendations from the CDC.
The ensuing resistance by blood banks to implementing the CDC’s donor screening measures is now viewed as a critical failure on their part in the effort to limit transmission of HIV early on in the epidemtic.
The second critical event would occur in December 15-16, 1983, when the Blood Products Advisory Committee of the FDA would convene a meeting to discuss all possible options of surrogate marker tests for HIV. This meeting is notable for being the CDC’s second attempt to address the need to implement blood screening as a means to implement safeguards to the blood supply.
In the year between the two meetings, blood banks would continue to collect donations from unscreened members of the public.
Representing four groups that CDC researchers identify as “most at risk” for HIV/AIDS, the four Hs are homosexuals, hemophiliacs, heroin users, and Haitians.
Learn More.
In the Morbidity and Mortality Weekly Report (MMWR) issued on this date, the U.S. Centers for Disease Control and Prevention (CDC) pointed to four distinct groups of people in the U.S. who were “at increased risk for developing AIDS.” According to the CDC, those groups were:
homosexual men with multiple sexual partners,
hemophiliacs,
abusers of intravenous drugs (i.e., heroin), and
Haitians (“especially those who have entered the country within the past few years”)
Many in the gay community co-opted the information, referring to it as “the 4H Club,” a sly redefining of its original meaning as a long-standing agricultural youth group.
The MMWR was published at a time when no effective treatment or cure for AIDS was available. People diagnosed with AIDS often had a few years — and sometimes just a few months — left before the disease would kill them.
Two months after this MMWR, the French virologist Luc Montagnier and his team at the Pasteur Institute in Paris would announce their discovery of the virus that causes AIDS. But at the time of this MMWR report, top U.S. researchers were still baffled by the disease and following leads that suggested that the deterioration of the immune system in AIDS patients was caused by a biological substance, likely passed from one person to another through blood.
“Available data suggest that the severe disorder of immune regulation underlying AIDS is caused by a transmissible agent,” the CDC states in its report.
The CDC goes on to recommend that members of high-risk groups refrain from donating blood or plasma.
“As long as the cause remains unknown, the ability to understand the natural history of AIDS and to undertake preventive measures is somewhat compromised,” the CDC report states. “However, the above recommendations are prudent measures that should reduce the risk of acquiring and transmitting AIDS.”
May 1983
French Researcher Discovers AIDS-Causing Virus
French researchers Francoise Barre-Sinoussi and Jean-Claude Chermann identify the virus that “might be” responsible for AIDS, calling it “LAV” (lymphadenopathy associated virus).
Learn More.
The following year, U.S. researcher Robert Gallo announced he had found the “probable” cause of AIDS, the retrovirus HTLV-III. The two viruses — HTLV-III and LAV — turned out to be one and the same, and in May 1986 it became officially known as the human immuno-deficiency virus, or HIV.
Barre-Sinoussi made her discovery while under French virologist Luc Montagnier, and both would go on to win the 2008 Nobel Prize in Physiology or Medicine for identifying the AIDS virus. Barre-Sinoussi’s discovery ultimately led to the development of anti retroviral medications that have turned AIDS from a death sentence to a manageable chronic disease.
Barré-Sinoussi dedicated her career as a scientist and as an activist to halting the spread of AIDS. Being on the front lines of the AIDS devastation was, she admitted, “very tough psychologically.”
The pressure was so intense that, once antiretroviral therapy was discovered in 1996, Barré-Sinoussi fell into a depression, and pulled back from her public commitments. But she soon returned to the fight, often travelling around the world to meet with political leaders and healthcare providers seeking solutions to local epidemics.
“Like everybody, I have some times in my life when I’m pessimistic,” she said. “I wonder whether I should continue … Then I go and have a trip to Africa or Southeast Asia and have a small meeting with people affected by HIV, and I forget my mood. I say, ‘OK, let’s go on. Let’s continue. This is real life. Don’t think about yourself.'”
She currently directs the Regulation of Retroviral Infections Unit at the Pasteur Institute, which is still looking for a vaccine or a functional cure.
* * * * * * Sources:
The Nobel Prize, “Women Who Changed Science: Francoise Barré-Sinoussi”
CNN, “HIV discovery ‘will change your life forever’” by Jen Christensen, June 4, 2013
Nature magazine, “The discovery of HIV-1” by Sonja Schmid, November 28, 2018
PBS News Hour, “How the Discovery of HIV Led to a TransAtlantic Research War” by Dr. Howard Markel, March 24, 2020
Researchers from the National Institutes of Health convene at the Clinical Center in Bethesda, Maryland to receive an update on AIDS, led by Anthony Fauci, M.D.
Learn More.
Then the director of the National Institute of Allergy and Infectious Diseases, Dr. Fauci led a presentation that summarized what was currently known about AIDS.
The presentation’s corresponding paper was co-authored by Dr. Fauci with Abe Macher, M.D.; Dan Longo, M.D.; H. Clifford Lane, M.D.; Alain Rook, M.D.; Henry Masur, M.D.; and Edward P. Gelmann, M.D. Among the conclusions the researchers made were:
– The cause AIDS was unknown but likely due to “a transmissible agent, most likely a virus.”
– AIDS was spread “by sexual contact, particularly homosexual activity.”
– Blood-borne transmission was “the other major recognized form of spread of the disease.”
– It was “highly likely” that the disease could not readily spread through casual, nonsexual, non-blood-borne routes.
The paper considers the possibility that the disease may kill all who are infected with it, and calls it “one of the most extraordinary transmissible diseases in history.”
* * * * * * Source:
Annals of Internal Medicine | American College of Physicians, “Acquired Immunodeficiency Syndrome: Epidemiologic, Clinical, Immunologic, and Therapeutic Considerations” by Anthony S. Fauci, M.D., Abe M. Macher, M.D., Dan L. Longo, M.D., H. Clifford Lane, M.D., Alain H. Rook, M.D., Henry Masur, M.D., Edward P. Gelmann, M.D., January 1, 1984
July 25, 1983
Ward 5B: Inpatient AIDS Ward Opens in San Francisco
San Francisco General Hospital opens Ward 5B, the first dedicated inpatient AIDS ward in the U.S. The ward consists of all-volunteer caregivers and staff.
Learn More.
Ward 5B is the answer to a petition organized by psychiatric nurse Cliff Morrison, demanding compassionate, holistic care for AIDS patients in San Francisco. By August, the ward’s 12 beds are fully occupied.
Run by Morrison and an all-volunteer team, Ward 5B allowed patients to create their own family made up of friends and partners. The nurses recognized that many of the patients were isolated from their families or had long-term, though not legal, partners.
The ward was one of the first units in the country that allowed visitors at any time.
* * * * * * Source:
August 1, 1983
UCLA Researchers Push for Discovery of AIDS Cause
At a UCLA medical conference, Los Angeles researchers urge the scientific community to focus their work on identifying the cause of “acquired immunodeficiency syndrome.”
Learn More.
In a presentation to the conference led by Michael S. Gottlieb, M.D., the UCLA researchers highlighted critical issues surrounding new disease, including diagnosis methodology, screening of blood products, and treatment of opportunistic infections and cancers related to the illness. They emphasized that the prognosis for recovery in affected persons was dire, as there still was no effective treatment once the illness took hold.
Co-authoring the presentation with Dr. Gottlieb were Jerome E. Groopman, M.D.; Wilfred M. Weinstein, M.D.; John L. Fahey, M.D.; and Roger Detels, M.D.* * * * * * Source:
August 1983
‘AIDS Memorandum’ Created for Research-Sharing
The National Institute of Allergy and Infectious Diseases begins publishing an informal newsletter, the AIDS Memorandum, through which scientists can share unpublished research findings.
Learn More.
The publication lasts for two years, until mainstream scientific journals begin expediting publication for articles on AIDS.
* * * * * * Source:
September 2, 1983
AIDS Exposure Precautions Issued to Healthcare Workers
CDC publishes the first set of AIDS exposure precautions for healthcare workers.
Learn More.
In response to growing concerns about the potential for AIDS transmission in healthcare settings, CDC publishes occupational exposure precautions for healthcare workers and allied health professionals.
* * * * * * Source:
September 9, 1983
CDC Rules Out AIDS Transmission by Casual Contact
In an MMWR article read around the world, CDC rules out transmission of AIDS by casual contact, food, water, air, or environmental surfaces.
The National Institute of Health hosts “A Workshop on the Epidemiology of AIDS” at the Holiday Inn Crowne Plaza in Rockville, Maryland.
Learn More.
At the workshop, researchers collaborated to develop recommendations for research on the epidemiology and natural history of AIDS, and exchange information and educate clinical investigators about epidemio logical study design.
Held over two days, the workshop featured several panel discussions and lectures, including “Summary of Epidemiological Research on AIDS Supported by the NIH” by Robert Edelman, MD, Clinical Professor of Medicine and Pediatrics, University of Maryland School of Medicine.
* * * * * * Source:
November 1983
Pediatric AIDS Cases Presented to NY Academy of Science, and Rejected
Dr. Arthur J. Ammann presented case reports of immunodeficiency in infants as evidence of AIDS infecting children — but the medical community largely refused to accept the idea that a disease spread among gay men was being found in babies.
Learn More.
Dr. Arthur J. Ammann traveled from San Francisco to New York City for an immunology conference hosted by the New York Academy of Science to report his research on pediatric AIDS patients, which discovered that HIV/AIDS can also be transmitted in utero – from mother-to-infant, and through blood transfusions.
Some conference attendees responded to Dr. Ammann’s presentation with indifference and rejection. Dr. Ammann said, “People just don’t want AIDS to affect infants, they just don’t believe it.”
Included in the nay-sayers was his former mentor, Robert A. Good, M.D., who had served as president of the American Association of Immunologists and more recently as director of the Sloan-Kettering Institute for Cancer Research.
“Bob Good got up and said that he didn’t think that we were seeing AIDS in children, that he had seen this immunodeficiency with CMV [cytomegalovirus virus] before,” Dr. Ammann recalled for the San Francisco AIDS Oral History Series. “I quickly responded, because I had looked up all the literature. I said, ‘If it’s been seen before, no one’s ever reported it.'”
Dr. Ammann said his early theory about pediatric AIDS was reinforced by a meeting he had with Arye Rubinstein, M.D., a New York City immunologist working with pediatric patients, who told him that he was receiving the same immediate resistance to his own case reports.
As the lead pediatric AIDS practitioners on the West Coast and East Coast, respectively, Drs. Ammann and Rubinstein did not let the initial rejection from the medical community deter them from their work. In fact, both would be later recognized for their important discoveries.
Dr. Ammann would serve as director of research for the Pediatric AIDS Foundation, a board member and President of amfAR, and on the Presidential National AIDS Task Force on Drug and Vaccine Development. In 1997, he would found Global Strategies for HIV Prevention to address the inequity of HIV prevention services provided around the world.
In a 1988 article for TheSan FranciscoChronicle, Dr. Ammann would draw nationwide attention to the issue of pediatric AIDS when he predicts that at least 20,000 children will contract AIDS in the next four years. Sadly, his prediction would be borne out. By 1992, about 5,000 cases of pediatric AIDS would be reported to the CDC, with the actual number of HIV-infected children to be estimated at about 20,000.
By 1985, Dr. Rubinstein would estimate that he had treated about 100 children with the AIDS virus at his practice based out of Albert Einstein College of Medicine in the Bronx.
At the time, New York public health policy dictated that pediatric AIDS patients be confined to hospitals, so misunderstood was the nature of the virus. So Dr. Rubinstein decided to open a day care center at Albert Einstein College for the families of pediatric AIDS patients, and successfully petitioned the City of New York for the funding to build it.
He would take personal risks to come to the defense of his pediatric patients’ parents, many of whom had a history of drug use and sex work, and were not equipped to navigate the backlash of fear and anger directed at them.
“I was almost assaulted after testifying in court in Brooklyn,” recalled Dr. Rubinstein in an 2011 edition of Einstein Magazine. “The parents in one school wanted to remove children who were infected, but I testified that HIV was not transmitted through casual contact. The parents got very upset, to the point where I had to be hauled out of the courtroom through a back door.”
In 1986, Dr. Rubinstein and colleagues would show that IV gamma globulin helps prevent infections and T-cell attrition in children with AIDS, significantly improving survival rates. Later the same year, he would demonstrate that in pregnant women with HIV, transmission of the virus often occurs in utero and not just at delivery or through breast-feeding.
In the April 1987 edition of Pediatric Research, he would co-author a paper about the increase in AIDS cases of women whose only known risk factor was heterosexual contact with HIV-positive men. In another pediatric publication, he would report that the leading cause of death in 1987 for women between the ages of 24 and 35 was AIDS.
In 1989, Dr. Rubinstein would launch a summer camp in the Catskills for children with HIV and their families (many more similar camps would open in the 1990s). He currently is chief of the Division of Allergy & Immunology at Children’s Hospital in Montefiore and Professor of Pediatrics at Albert Einstein College of Medicine.
November 22, 1983
WHO Brings Global Eye to Pandemic
The World Health Organization (WHO) holds its first meeting to assess the global AIDS situation and plan the international surveillance of the disease.
Learn More.
WHO’s meeting in Geneva marked the first time health officials representing countries from around the world met to share knowledge on risk factors, possible causes, and the clinical and immunological picture of potential spread of the new disease. Up until that point, only regional meetings of surveillance groups and researchers had convened in the U,S, and Europe to assess the problem and to exchange information, according to The Fourth Ten Years of the World Health Organization.
From the inaugural meeting on AIDS, preliminary recommendations were issued for prevention, diagnostic and screening tests, and clinical management of cases. Health officials also proposed areas of research and agreed to open a WHO center in Paris to coordinate global surveillance of the disease.
Following the meeting, WHO began reporting on AIDS cases and shared information through its publications about disease patterns, the risks of acquiring the disease, and methods of prevention and control.
December 15, 1983
FDA Hosts Conference to Consider Protections of Blood Supply
The CDC and FDA would convene a meeting of blood services organizations to discuss screening options for HIV/AIDS. This is the CDC’s second attempt to address the need for blood screening as a means to safeguard to the country’s blood supply.
Learn More.
At the December 15-16 meeting, the FDA’s Blood Products Advisory Committee facilitates a discussion of the options for HIV surrogate marker tests. This conference is a follow-up to the one held in January 1983, where blood bank scientists remained unmotivated to begin blood screening.
After the January meeting, an American Red Cross interoffice memo stated, “CDC is likely to continue to play up AIDS. It has long been noted that CDC increasingly needs a major epidemic to justify its existence.”
In the year between the two meetings, blood banks would continue to collect donations from unscreened members of the public. The initial resistance by blood banks to implement the CDC’s donor screening measures is now viewed as a critical failure on their part in the effort to limit transmission of HIV early on in the epidemtic.
At the December 1983 meeting, industry representatives proposed the creation of a task force to deliberate the details of a recommendation made at the meeting by Dr. Dennis Donohue, director of the FDA’s Division of Blood and Blood Products. Dr. Donohue proposed that hepatitis B anti-core testing be incorporated for routine plasma screening, since it would identify 90% of all potentially infectious or high-risk donors.
While Dr. Donohue was not enthusiastic about the task force approach, which was generally seen as the industry’s way to delay screening requirements, he agreed to it.
April 23, 1984
Dr. Robert Gallo Identifies Retrovirus as Cause of AIDS
U.S. Department of Health & Human Services Secretary Margaret Heckler announces that Dr. Robert Gallo and his colleagues at the National Cancer Institute have found the cause of AIDS, a retrovirus they have labeled HTLV-3.
Learn More.
Heckler also announces the development of a diagnostic blood test to identify HTLV-3 and expresses hope that a vaccine against AIDS will be produced within two years.
Dr. Gallo and his research colleagues developed a process to mass-produce the retrovirus for the purpose of developing the tools needed to identify, treat and cure the disease that has afflicted more than 4,000 Americans to date.
The announcement follows the announcement by the Pasteur Institute in Paris of its discovery of LAV, which they say causes AIDS.
Heckler said she thought the two viruses ”will prove to be the same.”
July 13, 1984
CDC Cites IV Drug Use & Needle Sharing as AIDS Transmitter
U.S. Centers for Disease Control pubishes research demonstrating that avoiding injection drug use and reducing needle-sharing would help prevent the spread of HIV/AIDS.
October 9, 1984
NYT Article Erroneously Suggests AIDS Transmission via Saliva is Possible
The New York Times reports that new scientific evidence has raised the possibility that AIDS may be transmissible through saliva . It will be another two years before proof emerges that this is false.
Learn More.
Epidemiologic studies to date point to sexual contact as well as transfusions of blood or blood products as the major risk factors leading to AIDS.
”Right now epidemiological studies do not point to saliva as the key mode of spread of AIDS and data show that close contact is much more important,” Dr. Robert C. Gallo, a leading AIDS researcher, told The New York Times.
Even so, this article spread fear among the public and further stigmatized those living with AIDS.
November 24, 1984
Fauci: Spread of AIDS is Accelerating
The spread of AIDS worldwide is accelerating, researcher Anthony Fauci, M.D., tells clinical staff gathered at an internal conference at the National Institutes of Health.
Learn More.
Dr. Fauci, who previously reported that the disease struck primarily gay men, tells his colleagues: “There is increasing evidence, particularly from Zaire, that the virus can be spread by heterosexual contact.”
Dr. Fauci’s presentation is accompanied by a paper co-authored with Henry Masur, M.D.; Edward Gelmann, M.D.; Phillip Markham, Ph.D.; Beatrice Hahn, M.D.; and H. Clifford Land, M.D.
In the paper, the scientists summarize the results of their research into the treatment of opportunistic infections.
“Attempts at immune reconstitution with lymphocytes and lymphokines have resulted in some transient improvement in immune function but without clinical effect, indicating the need for specific antiretroviral therapy in combination with immune reconstitution,” the paper states.
December 7, 1984
AIDS Conference Held in Irvine, California
Researchers and health officials convene on Dec. 7-8 in Irvine, CA for the International Conference on AIDS Associated Syndromes.
Learn More.
The conference brought together AIDS researchers conducting studies on the human immunodeficiency virus (HIV), which was then a new discovery.
At the time, no effective antiviral drugs for HIV/AIDS existed and research subjects typically died of AIDS-related illnesses within 10 years of infection with the virus. Researchers worldwide were scrambling to find a way to stop the AIDS virus from replicating within the body, according to the National Institutes of Health’s website for its Cancer Research Center.
The 1983 discovery of the AIDS virus by Luc Montagnier, M.D. at the Pasteur Institute in Paris (which was confirmed in 1984 by Robert Gallo, M.D. of the U.S. National Cancer Institute) had researchers all over the world searching for an effective treatment and cure to counter the quick spread of the new disease. Still more scientists were engaged with developing a vaccine for HIV — something that still eludes them to this day.
In December 1984, scientists at the forefront of this research gathered in southern California to try to answer the life-and-death questions of the day:
Was HIV alone responsible for AIDS, or was it activated by a combination with other factors in the way that other viruses — like Epstein-Barr virus or Cytomegalovirus — did.
What was the relationship of HIV to Kaposi’s sarcoma (since Kaposi’s sarcoma in AIDS could not be explained on the basis of the underlying immune deficiency)?
Where and how did the virus originate?
What were the clinical, cellular, and/or serological markers that determined the outcome of HIV infection?
Conference presentations also included work on identifying characteristics of early-stage AIDS and various treatment theories, and the specific ways in which HIV and AIDS exhibited in infants.
CDC Updates AIDS Definition & Issues Guidelines for Blood Screening
The U.S. Centers for Disease Control (CDC) revises the AIDS case definition to note that AIDS is caused by a newly identified virus. CDC also issues provisional guidelines for blood screening.
Learn More.
The report includes the following “recommendations for the individual” judged most likely to have an HTLV-III infection:
1. The prognosis for an individual infected with HTLV-III over the long term is not known.
However, data available from studies conducted among homosexual men indicate
that most persons will remain infected.
2. Although asymptomatic, these individuals may transmit HTLV-III to others. Regular
medical evaluation and follow-up is advised, especially for individuals who develop
signs or symptoms suggestive of AIDS.
3. Refrain from donating blood, plasma, body organs, other tissue, or sperm.
4. There is a risk of infecting others by sexual intercourse, sharing of needles, and possi
bly, exposure of others to saliva through oral-genital contact or intimate kissing. The efficacy of condoms in preventing infection with HTLV-III is unproven, but the consis
tent use of them may reduce transmission.
5. Toothbrushes, razors, or other implements that could become contaminated with
blood should not be shared.
6. Women with a seropositive test, or women whose sexual partner is seropositive, are
themselves at increased risk of acquiring AIDS. If they become pregnant, their offspr
ing are also at increased risk of acquiring AIDS.
7. After accidents resulting in bleeding, contaminated surfaces should be cleaned with
household bleach freshly diluted 1:10 in water.
8. Devices that have punctured the skin, such as hypodermic and acupuncture needles,
should be steam sterilized by autoclave before reuse or safely discarded. Whenever
possible, disposable needles and equipment should be used.
9. When seeking medical or dental care for intercurrent illness, these persons should
inform those responsible for their care of their positive antibody status so that ap
propriate evaluation can be undertaken and precautions taken to prevent transmission
to others.
10. Testing for HTLV-III antibody should be offered to persons who may have been infect
ed as a result of their contact with seropositive individuals (e.g., sexual partners, per
sons with whom needles have been shared, infants born to seropositive mothers).
March 2, 1985
Blood Test for HIV Becomes Available
The U.S Food and Drug Administration licenses the first commercial blood test, ELISA, to detect HIV. Blood banks begin screening the U.S. blood supply.
Learn More.
A positive result on ELISA (an enzyme-linked immunosorbent assay) must be confirmed by a second test for a person to receive a definitive diagnosis of HIV infection.
Today, many single-test options are available to test for HIV (Human Immunodeficiency Virus), including an FDA-approved, at-home test called OraQuick. Approved in 2012 for sale to anyone age 17 and older, the OraQuick In-Home HIV Test tests fluid from the mouth and delivers results in 20 to 40 minutes. The kit does not require sending a sample to a lab.
HIV screening is covered in the U.S. by health insurance without a co-pay, as required by the Affordable Care Act. Some testing sites offer free tests for those without medical insurance coverage.
The FDA still regulates the tests that detect infection with HIV. An estimated 1.1 million people in the U.S. are living with HIV, and about one in seven don’t know they have it, according to the CDC.
The CDC recommends that everyone between the ages of 13 and 64 years old be screened for HIV at least once as part of their routine health care. More frequent testing is recommended for people who have a higher risk of infection because of behaviors such as having sex without condoms, having sex with multiple partners, or injecting drugs using shared needles.
More than 2,000 researchers gathered at the conference to share information and assess prospects for controlling the disease, not yet realizing that the worst was yet to come.
The Atlanta conference featured 392 presentations and generated considerable excitement among participants eager to learn about how this new disease was playing out within specific populations in the U.S.
Much of the news was discouraging, however, as presenters introduced new data that showed that many of those dying in 1985 had been infected before 1981, and that within especially vulnerable populations, the epidemic was becoming entrenched.
At a side meeting before the day the conference opened, gay activists protested Reagan administration proposals to implement mandatory HIV testing policies, arguing that this would do little to halt the spread of the disease and would only intensify discrimination against vulnerable groups.
April 10, 1985
Haitians Removed from CDC’s High-Risk List
CDC removes Haitians from the list of those at increased risk for AIDS, because scientists can no longer justify including them on statistical grounds,
Learn More.
The CDC, which began investigating the mysterious and often-fatal disease in 1981, initially identified Haitian immigrants, intravenous drug users, hemophiliacs, and homosexual or bisexual men as groups at high risk for HIV/AIDS.
The CDC’s weekly reports of AIDS statistics included all four groups, but starting in April 1985, Haitians were no longer included as a separate listing.
The April 1985 report cited a total of 9,405 cases of AIDS reported in the U.S. Of those cases, 285 (about 3%) were Haitians, said Dr. Walter Dowdle, director of the Center for Infectious Diseases. Previously the rate for Haitians had been as high as 5%. By contrast, about 75% of the cases were of males who identified as homosexual or bisexual.
”The Haitians were the only risk group that were identified because of who they were, rather than what they did,” he said.
September 25, 1985
WHO: AIDS is ‘Major Public Health Problem’ around the World
Health officials from the AIDS Centers set up by the World Health Organization (WHO) affirm that the disease was now a major public health problem in several countries of the developed and developing world.
Learn More.
At a two-day convening in Geneva, Switzerland of representatives from WHO’s global centers on AIDS, health officials reviewed the epidemiologic status of AIDS world wide: more than 15,000 cases were reported in 40 countries, with 13,000 of the cases coming from the U.S.
WHO officials estimated that the number of cases in the U.S. would double to 26,000 in 1986, according to the Morbidity & Mortality Weekly Report issued by the U.S. Centers for Disease Control and Prevention on November 8, 1985.
WHO organized the meeting to review information presented at the International Conference on AIDS, held in Atlanta in April 1985, and assess the global implications.
According to The Fourth Ten Years of the World Health Organization, a key outcome of the WHO meeting was the decision to develop a comprehensive AIDS program in which WHO’s AIDS-focused collaboration centers would take an active part. WHO officials attending the meeting also decided to set up additional collaborating centers that focused on AIDS, in an effort to lay the surveillance groundwork needed for the proposed program.
WHO Director-General Halfdan Mahler expressed concern regarding AIDS, but in separate comments to the media, he said he considered other diseases to be top priority outside the U.S.
“AIDS is not spreading like a bush fire in Africa,” Mahler said in widely reported accounts. “It is malaria and other tropical diseases that are killing millions of children every day.”
December 6, 1985
CDC Issues Precautions to Prevent Mother-to-Infant Transmission
The CDC’s Morbidity and Mortality Weekly Report recommends that HIV-infected women delay pregnancy until more is known about the risks of transmission, and advised new mothers to avoid breastfeeding.
Transmission of the virus during pregnancy or labor and delivery is demonstrated by two reported AIDS cases occurring in children who had no contact with their infected mothers after birth.
With studies on the subject of pediatric AIDS just beginning, the rate of perinatal transmission of HIV from infected pregnant women is unknown and the limited amount of available data suggests a high rate.
However, the report contends that perinatal transmission (from an infected mother to her newborn) is not inevitable.
Of three children born to women who became infected with HIV by artificial insemination from an infected donor, all were in good health and negative for antibody to the virus more than 1 year after birth. Another child, born to a woman living with AIDS, was HIV-negative and healthy at birth and at 4 months of age.
In December 1985, a total of 217 cases of AIDS have been reported among children under age 13, and 60% of them have died.
The CDC report states that, on average, people diagnosed with AIDS die about 15 months after the disease is diagnosed. The report also shows:
Between 6/1/1981 and 1/13/1986, there have been 16,458 cases of AIDS (16,227 adults and 231 children) reported in the U.S. Of these, more than half of the infected people have died.
The number of cases reported each 6-month period continues to increase.
Cases have been reported from all 50 states, the District of Columbia, and three U.S. territories.
“One million Americans have already been infected with the virus, and this number will jump to at least 2 million or 3 million within 5 to 10 years,” National Institute of Allergy and Infectious Diseases (NIAID) Director Anthony Fauci tells The New York Times.
April 21, 1986
Scientists Discuss Safety of Blood Products at WHO Meeting
About 160 scientists attended a meeting in Geneva hosted by the World Health Organization (WHO) to discuss the safety of blood and blood products and antibody screening issues in relation to AIDS.
Learn More.
The meeting’s main conclusion was that the risk of transmitting HIV by factor VIII or factor IX concentrates, commonly used to treat hemophilia, could be reduced or eliminated with proven methods of screening for HIV antibodies and inactivation, according to The Fourth Ten Years of the World Health Organization.
The meeting, which included scientists from 15 countries, also presented goals for WHO’s Program on AIDS, including the creation of a global surveillance system to monitor HIV infection as well as deaths from AIDS-related illness.
Representing the U.S. were Kenneth J. Bart, M.D., the health director for the U.S. Agency for International Development; William C. Bartley, the international health attaché for the U.S. Mission to the United Nations; and Walter R. Dowdle, Ph.D., director of infectious disease at the Centers for Disease Control and Prevention, according to the meeting report.
May 1, 1986
AIDS Virus Officially Called ‘HIV’
The International Committee on the Taxonomy of Viruses announces that the virus that causes AIDS will officially be known as “Human Immunodeficiency Virus ” (HIV).
Learn More.
An international committee of scientists is proposing that the AIDS virus be called by a new name: human immunodeficiency virus, or HIV.
Until now, the closely related variations of the virus have been most frequently referred to as HTLV-3, for human t- cell lymphotropic virus type 3, or LAV, for lymphadenopathy associated virus.
HTLV-3 is the designation given by Dr. Robert Gallo and colleagues at the National Cancer Institute, co-discoverers of the virus and leaders in the American research effort. LAV is the name used by Dr. Luc Montagnier and associates at the Pasteur Institute in Paris, also credited as discoverers of the virus.
October 1986
AIDS Health Services Program Launches in 11 U.S. Cities
The AIDS Health Services Program launches with $17.2 million in funding for patient-care projects in 11 major cities.
The goals of the program are to develop community-based services for persons with AIDS and to determine factors that facilitate or impede service.
The foundation starts with nine projects located in 11 communities: Atlanta, Dallas, Fort Lauderdale, Miami, Nassau County (NY), New Orleans, Newark, Jersey City, Seattle, and West Palm Beach.
The AIDS epidemic in each site varies substantially. Lack of health insurance represents a problem for the majority of clients in states having the most restrictive Medicaid policies (Atlanta, New Orleans, and Dallas) and in communities where a large proportion of clients enter the program before their condition progresses to AIDS (Miami, Fort Lauderdale, and West Palm Beach).
Between 1987 and 1990, the average annual population with AIDS in program sites increase 126% (with increases ranging from 91% to 175%). During that period, the average increase in the number of persons alive with an AIDS diagnosis in these eleven cities is 191%, ranging from 181% to 257%.
The men and women attempting to build a network of coordinated services for persons with HIV/AIDS find themselves with an extremely difficult task. As the epidemic progresses, there is a substantial increase in the scope of the epidemic as well as change in the racial, sex, and risk-group composition of HIV-infected persons.
Program staff have to cope with confusing state and federal policy, complicated by changes in medical treatment and in the conceptualization of AIDS. In 1986, AIDS is still perceived as an acute, fatal illness, and policies for expanding terminal care benefits are the focus of discussion. However, soon the focus would shift to early intervention and ongoing treatment programs for a new chronic disease.
April 29, 1987
Western Blot: FDA Releases Updated HIV Test
FDA approves a new, more specific test for HIV antibodies, the Western blot blood test kit.
Learn More.
For several years, the HIV-1 Western blot would be considered the “gold standard” for laboratory diagnosis of HIV-1 infection, but is no longer recommended. The two main reasons for this are the inability of the Western blot to detect acute infection and the potential to misclassify HIV-2 infection as an HIV-1 infection.
A report in Nature in June 1993 would conclude that researchers need to “reappraise” the use of the Western blot antibody tests as a diagnostic and epidemiological tool for HIV infection.
August 14, 1987
CDC Updates Guidelines for Counseling & Antibody Testing
The CDC releases guidelines for public health agencies to help them reduce fear and concerns as they implement HIV testing programs. The report encourges agencies to target outreach to at-risk populations and strengthen policies for patient confidentiality.
Per the guidelines, health agencies should endeavor to provide ready, confidential access to HIV testing to those most at risk of HIV infection.
As examples, the report cites programs offering counseling and testing to gay men, IV-drug users, persons with hemophilia, the sexual and/or needle-sharing partners of these persons, and patients of sexually transmitted disease clinics.
The report also addresses the issue of false-positive HIV test results and its impact, stating that most false-positives are due to human error and more precautions should be used by medical personnel to ensure the accuracy of results.
“All laboratories should anticipate the need for assuring quality performance of tests for HIV antibody by training personnel, establishing quality controls, and participating in performance evaluation systems,” the report advises.
August 21, 1987
Universal Precautions Introduced to Medical Environment
CDC updates its recommendations for the prevention of HIV transmission in healthcare settings, calling for medical workers to practice universal precautions.
Learn More.
The report emphasizes the need for healthcare workers to consider all patients as potentially infected with HIV and/or other blood-borne pathogens and to adhere rigorously to infection-control precautions for minimizing the risk of exposure to blood and body fluids of all patients.
The CDC defines healthcare workers as “persons, including students and trainees, whose activities involve contact with patients or with blood or other body fluids from patients in a healthcare setting.”
Universal precautions are listed in the report, along with precautions for invasive procedures, dentistry, dialysis, laboratory procedures, and autopsies and mortuary work.
November 13, 1987
AMA Declares Ethical Obligation to Treat PWA’s
The American Medical Association declares that doctors have an ethical obligation to care for people with AIDS, as well as for those who have been infected with the virus but show no symptoms.
AMA ethics council also tells physicians that if a patient carrying the AIDS virus refuses to discontinue dangerous sexual practices, a doctor should notify public health authorities and even take it upon himself to directly inform individuals who may be in danger of infection.
The new AMA strictures conflict with California law, under which it is illegal for a doctor, without the patient’s consent, to tell anyone a person has tested positive for the AIDS virus or has AIDS.
The AMA states that no evidence exists that large numbers of doctors have refused to treat patients who tested positive for the AIDS virus.
But an AMA spokesperson concedes, “There have been physicians who have chosen to make public statements that they will not treat HIV-positive people. Those statements have generated tremendous amounts of discussion and debate.”
February 12, 1988
First AIDS Drug Released under New FDA Rules
Trimetrexate becomes the first AIDS drug given pre-approval distribution status under new FDA regulations.
Learn More.
Trimetrexate was used to treat pneumocystis carinii pneumonia in AIDS patients who could not tolerate standard treatments.
May 6, 1988
New Study: Human Saliva Prevents Spread of AIDS Virus
A new study suggests that human saliva contains substances that prevent the AIDS virus from infecting white blood cells.
Learn More.
In the study, published in the May issue of The Journal of the American Dental Association and reported widely in the media, the researchers tested saliva from three healthy men aged 35, 40 and 42. Researchers determined that the subjects were not infected by HIV and they were not known to be at high risk of infection.
The researchers said the finding might help explain why no cases have been documented in which the AIDS virus was transmitted from person to person through saliva.
The research was led by Philip Fox, M.D., who cautioned that the study results do not eliminate the possibility of HIV infection from oral sex or deep kissing. Dr. Fox explained that the virus could enter the bloodstream through cuts in the mucous membranes that line the mouth or it might be able to infect cells on the surface of mucous membranes.
UT researchers Samuel Baron, Joyce Poast and Miles W. Cloyd sought to confirm the results of Fox’s 1988 study and subsequent studies that showed that proteins in saliva seem to neutralize or disable the AIDS virus, Published in the Archives of Internal Medicine, the UT study would indicate that saliva inactivates more than 90% of the HIV-infected blood cells by breaking the virus apart into non-infectious components.
June 1988
U.S. Launches Study on Transmission in Women & Infants
An epidemiologic study of HIV transmission during pregnancy and birth is launched by the National Institute of Allergy and Infectious Diseases and the National Institute of Child Health and Human Development.
Learn More.
The Women and Infants Transmission Study (WITS) captured data on the natural history of HIV infection in pregnant women and their infants. The study followed the women with their infants through the infants’ first few years of life.
Conducted at obstetric/gynecologic and pediatric clinics in Boston, Chicago, Manhattan, Brooklyn, Houston, and San Juan, the first phase of the study captured data from 788 HIV-infected pregnant women and 657 infants born to them.
Of the women studied in the initial phase of the trial, 82% were women of color, which was intentionally representative of infected women in the U.S. The researchers found they needed to be resourceful in finding ways to retain participants, because many in the cohort had low incomes and histories of substance abuse.
In 1993, WITS would receive another $5 million in funding and expand to include participants from additional cities. Over the years, data collected from WITS would become instrumental in determining treatment and transmission prevention strategy for women and infants.
August 1988
Volunteers Enroll in Clinical Trials for HIV Vaccine
National Institute of Allergy and Infectious Diseases, headed by Anthony Fauci, M.D., creates the first U.S. cooperative HIV vaccine clinical trials group and begins enrolling volunteers.
Learn More.
NIH established the Office of AIDS Research (OAR), which then launched the AIDS Vaccine Evaluation Group (AVEG) to oversee the first study of an experimental AIDS vaccine.
At the time, researchers and the medical community were hopeful that a vaccine would be quickly developed and rolled out to the general public. But in spite of the optimism expressed by many, Dr. Anthony Fauci published a Public Health Report that warned that developing a HIV vaccine would be difficult. Dr. Fauci listed the following as issues that complicate the development of an effective AIDS vaccine:
– the lack of “an appropriate animal model for AIDS,”
– the absence of a defined protective immune response in persons infected with HIV,
– the long latent period between initial infection and the development of symptoms,
– the existence of multiple strains of HIV, and
– the spread of HIV by way of cell-associated virus.
“When HIV was discovered and established as the cause of AIDS in 1983–1984, many people believed that a vaccine would be easily developed and rapidly deployed. After all, vaccinologists had been very successful in developing vaccines for a whole range of viral diseases,” José Esparza of the Bill and Melinda Gates Foundation wrote in 2013. “However, the paradigm that allowed the development of most existing viral vaccines, which is based on the recreation of the protective immunity that develops after natural infection, does not work in the case of HIV.”
Still today, scientists continue their quest to develop a vaccine. Extensive studies are underway to determine how HIV is able to avoid the immune responses spurred by vaccines. In an article for the Association of American Medical Colleges, David Diemert, M.D. explained the challenge.
“From the very second HIV infects a person, it starts to escape from the immune response,” said Dr. Diemert, clinical director of vaccine research at the George Washington University School of Medicine and Health Sciences.
November 25, 1988
CDC Study: One of Every 500 College Students Infected with HIV
One out of every 500 college students are infected with HIV, according to a new study released by the Centers for Disease Control and Prevention.
Learn More.
As part of its series of HIV surveys and studies, the CDC collaborated with the American College Health Association to assess HIV infection in college students. For the first 12,000 students tested, a seroprevalence of HIV of 0.2% was found. The majority of seropositive specimens came from male students.
The tests were conducted anonymously on blood specimens drawn from students at student clinics. The initial results came from student specimens from 17 of 19 participating campuses. The researchers stated that the survey did not include a random sampling of all college students, just students who had blood drawn at their campus health center.
The researchers conclude that “these results demonstrate that HIV infection and the potential for its transmission are present on many college campuses.” They interpret the data to mean that older students and men are at greatest risk in this population.
The colleges participating in the study were:
Central Missouri State University
Emory University
Mississippi State University
Northwestern University
Rutgers University
San Diego State University
Southern Illinois University
University of California – Berkeley
University of Colorado
University of Connecticut – Storrs
University of Georgia
University of Kansas
University of Maryland – Baltimore County
University of Maryland – College Park
University of Massachusetts – Amherst
University of New Hampshire
University of Southern California
University of Texas – Austin
University of Washington
February 20, 1989
Doctor Skirts NIH Delay in PCP Treatment Protocol
When a CDC statistician tells AIDS activist Michael Callen that 30,534 Americans have died of AIDS-associated Pneumocystis pneumonia (PCP), Callen’s physician responds with information indicating that many of these deaths could have been prevented with existing (but “unapproved”) treatment.
Learn More.
Dr. Joseph Sonnabend, Callen’s doctor, would later write about treatment to prevent PCP with “a drug that had been known to prevent this kind of pneumonia since 1977.”
The doctor would blame NIH Director Dr. Anthony Fauci for the delay in this treatment being available on a widespread basis, saying that Dr. Fauci “wanted data from a clinical trial of Bactrim for PCP prophylaxis in AIDS before he would recommend its use.”
Dr. Sonnabend says he refuses to wait for the NIH to collect data and reach its conclusions, revealing that he is already prescribing Bactrim (also known as Septra, Septrin or co-trimoxazole) and Dapsone to patients he routinely deems to be at risk for PCP, with positive results in his patients.
Years later, looking back at this time, Dr. Sonnabend would write: “People were dying of PCP at a terrifying rate; I and some other physicians could not wait for these recommendations.”
March 1989
WHO Estimates Total AIDS Cases Worldwide at 400,000
Reported AIDS cases total 142,000 in 145 countries. However, the World Health Organization estimates that there are as many as 400,000 cases worldwide.
June 16, 1989
CDC Issues Treatment Guidelines for PCP Prevention
The U.S. Centers for Disease Control and Prevention issues the first guidelines for preventing Pneumocystis cariniipneumonia, known as PCP, an infection which often leads to the severe illness and death for people living with AIDS.
Learn More.
The guidelines recommend a regimen of two compounds to prevent the onset of PCP: trimethoprim-sulfamethoxazole and pentamidine. The CDC bases its recommendations on a study of 60 adults living with AIDS, which suggest that those who received treatment have fewer episodes of PCP and lived longer, compared with untreated patients.
Trimethoprim-sulfamethoxazole, a combination of the antibiotics sulfamethoxazole and trimethoprim, commonly causes side effects in patients that include nausea, vomiting, diarrhea, and loss of appetite.
Pentamidine, given as an aerosol in a nebulizing device, commonly causes adverse effects including coughing, difficulty breathing, difficulty swallowing, and chest pain or congestion.
The Public Health Service recommends physicians to start this treatment with:
any HIV-infected adult patient who has already had an episode of PCP, and
those whose CD4+ cell count is less than 200/mm3 (or less than 20% of total lymphocytes).
CD4+ cells would soon be referred to as “T-helper” or “T4 cells,” because one of their main goals is to send signals to other kinds of immune cells, which then destroy infectious particples.
Patients with CD4+ cell counts of less than 100/mm3 (or less than 10%), as well as patients with oral thrush or persistent fever, are at particularly high risk for PCP, the report states.
According to HIV.gov, a healthy T cell count should be between 500 and 1,600 T cells per cubic millimeter of blood (cells/mm3).
June 23, 1989
CDC Updates Guidelines on Transmission Prevention for Healthcare Workers
The Centers for Disease Control releases updated guidelines to help prevent the transmission of HIV and Hepatitis to healthcare and public safety workers.
Learn More.
The guidelines are a response to recently enacted legislation, the “AIDS Amendments of 1988” in the HOPE Act of 1988, passed by Congress and signed by President Ronald Reagan on Nov. 4, 1988.
The legislation calls for the Secretary of Health and Human Services, acting through the Director of the CDC, to “develop, issue, and disseminate guidelines to all health workers, public safety workers (including emergency response employees) … concerning methods to reduce the risk in the workplace of becoming infected with the etiologic agent for AIDS, and circumstances under which exposure to such etiologic agent may occur.”
The report states that, as of September 1988, a total of 3,182 (5.1%) of the 61,929 adults reported to be living with AIDS are employed in a healthcare setting. Of the healthcare workers with AIDS, the means of HIV acquisition is “undetermined” for 5% of them (169 workers), suggesting that infection occurred in the workplace.
Of these 169 health-care workers with AIDS, 44 are interviewed directly or have other background information available about their cases. The occupations of these 44 are:
nine nursing assistants
eight physicians, four of whom are surgeons
eight housekeeping or maintenance workers
six nurses
four clinical laboratory technicia)ns
two respiratory therapists
one dentist
one paramedic
one embalmer
four others who did not have contact with patients
Eighteen of these 44 health-care workers report parenteral (i.e., not delivered via the intestinal tract) and/or other non-needle-stick exposure to blood or other body fluids from patients in the 10 years preceding their diagnosis of AIDS. None of the exposures involve a patient with AIDS or known HIV infection.
June 26, 1989
Chief Researcher Calls for Access to Experimental Treatment
Dr. Anthony Fauci, head of the National Institutes of Health’s National Institute of Allergy and Infectious Diseases (NIAID), endorses giving HIV-positive people who do not qualify for clinical trials access to experimental treatments.
Learn More.
In a front-page article by Gina Kolata in The New York Times, Dr. Fauci calls for a new system that would allow patients far greater access to experimental drugs.
This marks a major turnaround in government policy, which restricts access to experimental drugs with the reasoning that patients would have no reason to join a clinical trial if they could get a drugs by other means.
Since his early involvement in developing treatment for HIV/AIDS, Dr. Fauci had adhered to the National Institutes of Health policy that research need not focus on the immediate welfare of patients.
“It was clear to me that Fauci was inclined to enforce the paternalistic medical tradition in which he had trained: doctors and scientists were unquestioned authorities, and drug development had to follow a rigid process that included animal testing and rigorous clinical trials. Otherwise, the benefits and the risks of these drugs could not be adequately assessed,” writes Michael Specter in his profile of Dr. Fauci for The New Yorker in April 2020. Specter covered the AIDS epidemic for the Washington Post in the 1980s.
AZT (azidothymidine) was the only approved drug available to treat HIV/AIDS, but it had harsh side effects. When new clinical studies began, involving cocktails of AZT and similar compounds, tens of thousands of people asked to participate. But volunteers were rejected if they used other experimental drugs. And many more didn’t have the means to get to facilities and practitioners conducting the clinical trials.
“They started becoming amazingly iconoclastic and confrontational, and that scared the hell out of the scientists, who were fundamentally quite conservative,” Dr, Fauci tells Specter in The New Yorker profile. “When they were demonstrating on the NIH campus, disrupting Wall Street, disrupting St. Patrick’s Cathedral, instead of listening to them, scientists withdrew.”
However, Dr, Fauci decided to look beyond the activists’ furious rhetoric and style, and began to listen to what they had to say.
“And what they were saying made absolutely perfect sense,” Dr. Fauci says.
Faced with mounting evidence that his cautious approach made no sense, he reversed himself and promoted activist demands for more access to experimental treatments.
In the process, “Fauci transformed from a conventional bench scientist into a public-health activist who happened to work for the federal government,” writes Specter.
August 18, 1989
AIDS Cases in U.S. Reaches 100,000
CDC reports that the number of reported AIDS cases in the United States has reached 100,000.
December 31, 1989
LA Times: Women & Infants Represent Key Groups Hit by HIV/AIDS in LA
The Los Angeles Times releases AIDS statistics that show that Los Angeles has more than twice as many female cases and three times as many pediatric cases as San Francisco.
Learn More.
In a column by Victor F. Zonana, the LA Times publishes newly released data that indicate that AIDS cases and deaths are rising dramatically and reaching new populations. New cases recorded between January and November 1989 (the most recent months data was available) of full-blown AIDS in Los Angeles County totaled 2,274, up 28% from a year earlier.
In addition, planning documents for LA County estimated that by 1992, the cumulative total number of cases would more than double, to at least 19,000, and could rise to as high as 44,000 cases.
Zonana, the LA Times columnist, posed the question: “Will [LA County] go the way of San Francisco, widely praised as a model of compassionate and cost-effective AIDS care? Or will Los Angeles resemble New York City, the third major center of the epidemic, where people are dying in the streets as the unchecked spread of the virus among drug addicts fills public and private hospitals beyond capacity?”
Zonana wrote that one of the unique challenges facing the LA community was the large population of Latinos, some of whom were undocumented and disconnected from health services, and the potentially adverse impact of Roman Catholic Church’s unyielding stand against the use of condoms.
Torie Osborn, then-director of the Gay and Lesbian Community Services Center (now the Los Angeles LGBT Center), expressed her concerns that members of the Latino community were particular at risk of HIV infection as a result of these church teachings.
“In the past two months, our clinic has found 45% (infection rates) among gay and bisexual Latinos,” said Osborn, compared to 17% among Anglo gays. “The figure just leaps out at you … it is really alarming.”
The following are selected AIDS statistics through Sept. 30, 1989 for New York, Los Angeles and San Francisco, the three major centers of the epidemic which together accounted for 34.5% of the nation’s AIDS cases.
The data shows that Los Angeles has more than twice as many female cases and three times as many pediatric cases as San Francisco, even though its total caseload is only 11% higher.
New York
Total cases: 22,571
Total deaths: 12,246
Children under 13: 536
Adult women: 2,934
Gay/bisexual contact: 10,916
Heterosexual IV drug use: 6,166
Reported new cases: 4,081
Year-to-date Total White cases: 39%
Year-to-date Total Black cases: 33%
Year-to-date Total Latino cases: 27%
Projected net municipal outlay*: $229.6 million
Los Angeles
Total cases: 8,063
Total deaths: 5,306
Children under 13: 70
Adult women: 244
Gay/bisexual contact: 6,474
Heterosexual IV drug use: 325
Reported new cases: 1,928
Year-to-date Total White cases:65%
Year-to-date Total Black cases: 16%
Year-to-date Total Latino cases: 18%
Projected net municipal outlay*: $20.5 million
San Francisco
Total cases: 7,277
Total deaths: 4,706
Children under 13: 22
Adult women: 91
Gay/bisexual contact: 6,164
Heterosexual IV drug use: 159
Reported new cases: 1,458
Year-to-date Total White cases: 82%
Year-to-date Total Black cases: 7%
Year-to-date Total Latino cases: 8%
Projected net municipal outlay*: $19.9 million
*for AIDS prevention and care, current fiscal year; does not include private contributions, state and federal expenditures or payments from private insurers.
The sources for the LA Times data were the Department of Geography, California State University, Northridge and Los Angeles County Department of Health Services.
January 26, 1990
U.S. Updates Guidelines for Reducing Healthcare Worker Exposure
On January 26, the U.S. Public Health Service issues a statement on managing occupational exposure to HIV, including considerations regarding post-exposure use of the antiretroviral drug, AZT.
Learn More.
The CDC issues a report reviewing the PHS recommendations for the management of occupational exposures that may place workers at risk of acquiring HIV infection, with a focus on those administering AZT treatment.
May 1, 1990
AIDS Cases Rising Among Heterosexuals
Cases attributed to heterosexual transmission are growing faster than any other category of AIDS cases, according to the U.S. Centers for Disease Control.
Learn More.
The CDC reports that from 1988 to 1989, AIDS cases caused by heterosexual transmission jumped 36%. Of the infected heterosexuals who are women, many give birth to infants who are also infected.
”The heterosexual epidemic is no myth,” Dr. Jerome Groopman, head of the AIDS program at Harvard’s New England Deaconness Hospital, told The New York Times. ”It is real.”
According to the CDC, about 128,319 cases of fully symptomatic AIDS were reported from 1981 through March 1990. Of those, CDC officials estimate that about 6,231 — 5% — have been cases in which the disease was transmitted by heterosexual sex.
The NYT article noted that federal statistics likely reflect an undercount of heterosexual transmission of AIDS, because the CDC’s reporting system is ”hierarchical,” meaning that AIDS cases were attributed to homosexual sex, intravenous drug use and all other risk categories first. Only those that did not fit into these categories were put in the “heterosexual transmission” category.
Thomas C. Quinn, an AIDS researcher at the National Institute of Allergy and Infectious Diseases, part of the National Institutes of Health, told the NYT that there is a rapid increase in heterosexually transmitted disease in several cities, especially those of the East Coast, including Newark, Philadelphia, Baltimore, Washington and Miami.
Dr. Quinn recently presented a paper at an AIDS conference at Johns Hopkins University, where he and his colleagues described syphilis as one of the key factors in spreading AIDS among heterosexuals in the inner city.
The NIAID researchers studied 4,863 patients in two inner city clinics in Baltimore that treat sexually transmitted diseases. Among the heterosexuals who said they did not use intravenous drugs, those who had syphilis were seven to nine times more likely to have AIDS than other patients at the clinic.
In December 1988, NIAID launched the Heterosexual AIDS Transmission Study (HATS) to collect data on male and female heterosexuals at high risk of AIDS who are not IV drug users.
CDC Report of HIV Transmission via Dentistry Alarms Public
The U.S. Centers for Disease Control and Prevention reports the transmission of HIV to a patient through a dental procedure performed by an HIV-positive dentist in Florida, releasing a wave of panic across America.
Learn More.
The CDC report described what it considered to be the first known case of clinical transmission of HIV: Kimberly Bergalis, a 19-year-old college student, underwent a molar extraction in December 1987. About two years later, she tested positive for HIV and the CDC was able to match the virus’ strain to that of her dentist, Dr. Jeffrey Acer.
Reported to the CDC by the Florida Department of Health and Rehabilitative Services (HRS), the case described Bergalis — who said she had never engaged in sexual intercourse — as having no identified risk factor for HIV infection and that, at some time following a wisdom tooth extraction performed by Dr. Acer, she became infected with HIV.
In an open letter to his patients, Dr. Acer wrote: “I am a gentle man, and I would never intentionally expose anyone to this disease. I have cared for people all my life, and to infect anyone with this disease would be contrary to everything I have stood for.”
The CDC suggested that during the dental procedures, “higher titers of virus may have been present in the dentist’s blood and he may have been more likely to transmit virus than earlier in the course of his HIV disease.”
Following the notification, two more of Acer’s former patients would test positive with a strain similar to his. In addition, a third infected patient would be identified by the Florida health department and a fourth would contact the CDC directly to report that she was HIV-infected and a former patient of the dentist.
The Florida health department would then reach out to 1,100 additional persons who potentially were patients of Dr. Acer to offer counseling and HIV-antibody testing. Of them, 141 were tested, and all results were negative. In addition, none of the dentist’s 14 employees tested positive for HIV.
Staff members of the dental office told HRS officials that barrier precautions had been introduced into the practice by early 1987 and that all staff, including the dentist, wore latex gloves and surgical masks for patient-care activities. Staff reported that they changed gloves and washed their hands between most patient contacts; occasionally, however, they washed gloves rather than changed them between patient contacts. Additionally, staff reported that by 1987, all surgical instruments were autoclaved.
Dr. Acer was diagnosed with symptomatic HIV infection in late 1986 and AIDS in September 1987. While he was in practice, he had no record of peripheral neuropathy, dementia, thrombocytopenia or other bleeding disorder, hand dermatitis, or injury.
Dr. Acer closed his practice in 1989 after his T-cell (CD4 lymphocyte) count dropped under 200. He would die on Sept. 30, 1990 at the Hospice of Palm Beach County at West Palm Beach with his parents at his side.
Kimberly Bergalis would spend her final years advocating for the mandatory testing of medical professionals. She is described as “the one AIDS patient the AIDS community will not embrace, a frightening and hostile new public symbol of an epidemic the AIDS community thought it had tamed.”
Larry Gostin, professor of health law at Harvard University, would tell The Washington Post in September 1991, “What Kimberly Bergalis symbolizes is … that AIDS is to be feared and that it can be contracted easily in health-care settings. She has created fear.”
“I’d like to say that AIDS is a terrible disease that you must take seriously. I did nothing wrong, yet I’m being made to suffer like this. My life has been taken away. Please enact legislation so that no other patient or health care provider will have to go through the hell that I have. Thank you.”
Bergalis would die of AIDS-related illness on Dec. 8, 1991 at the age of 23.
May 22, 1992
Rapid HIV Blood Test Gives Results in 10 Minutes
FDA licenses a rapid HIV diagnostic test kit which gives results from a blood test in 10 minutes.
As the only rapid enzyme immunoassay (EIA) approved for diagnostic use in the U.S., the test is manually performed by mixing a small amount of the patient’s blood with an antibody agent to which only HIV-1 antibodies will attach.
This test is considered by researchers to be part of the third wave of HIV tests, following the ELISA and Western Blot tests of the mid-1980s. A 1993 clinical trial analyzing almost 2,000 test samples would show the SUDS HIV-1 test to give false-positive results at a relatively high rate.
December 1992
#1 Cause of Death for Young Adult Men is AIDS
With the death rate from HIV infection steadily and dramatically increasing over the past 10 years, AIDS becomes the leading cause of death in the U.S. for men aged 25-44.
Learn More.
A report from the Centers for Disease Control announces that HIV infection emerged in the 1980s as a leading cause of death in the U.S., and now HIV infection is the number one cause of death among men aged 25-44 years.
The CDC bases this assessment on data obtained from death certificates filed in all 50 states and the District of Columbia. Statisticians suspect the magnitude is greater than indicated in the report.
The report also notes that HIV infection is more severely advancing to death for blacks and hispanics than other racial/ethnic groups.
“These differences probably reflect social, economic, behavioral, or other factors rather than race/ethnicity directly,” the report states. “The social and cultural context of HIV infection must be addressed through prevention efforts designed to meet the needs of specific communities.”
.
May 7, 1993
FDA Approves Female Condom
The U.S. Food and Drug Administration (FDA) approves the female condom, giving women a new way to protect themselves from sexually-transmitted diseases and unwanted pregnancy..
Learn More.
The condom, which is ma nufactured by Chartex International, becomes available over the counter at most major drug stores in Southern California, under the name Reality Female Condom.
Although the female condom gives women more options for birth control, it is slow to catch on with the general public.
Donna Diaz, a representative of Planned Parenthood of Los Angeles, tells California State University’s campus newspaper that the female condom is not popular because it is “more awkward to use” than the male condom.
“It’s not as effective as the male condom and it’s very inconvenient to use,” she says.
However, Holly Sherman, spokeswoman for The Female Health Company — which markets and distributes the condom — disagrees, saying the female condom provides protection from disease on genital areas because there is “less skin touching skin” and the chance of transmitting a disease is less likely.
The female condom has a sheath material and a flexible inner ring, and is inserted similar to a diaphragm. A woman squeezes the ring and inserts it as far as possible into the vagina. The ring then covers the cervix. Its sheath material holds the condom in place. The outer ring lines the vaginal wall and helps cover the lips of the vagina. The sexual partner must stay within the confines of the female condom or it’s ineffective.
August 1993
U.S. Launches Two Research Studies Focused on Women
The Women’s Interagency HIV Study and HIV Epidemiology Study begin; both are major U.S. federally funded research studies on women and HIV/AIDS.
Learn More.
The Women’s Interagency HIV Study establishes a multi-center, prospective, observational cohort study of women living in the U.S. who are either HIV-infected or at risk for HIV acquisition.
The program would play an important role in the National Institute of Allergy and Infectious Diseases’ effort to understand the current epidemiology of HIV infection, disease progression, treatment use and outcomes, and related co-morbidities among U.S. residents with HIV.
Understanding differences in HIV disease and treatment outcomes between women compared to men, and in different racial and ethnic groups, is a critical public health goal. The clinical research consortium is an integral part of the NIAID portfolio of research on HIV in women.
December 18, 1993
CDC Ties Definition of AIDS to T-cell Counts
The U.S. Centers for Disease Control and Prevention expands its definition of AIDS, declaring those with T-cell (CD4) counts below 200 to have AIDS.
Learn More.
In a report, the CDC revises its case definition of AIDS to emphasize the clinical importance of the CD4+ T-lymphocyte count in the categorization of HIV-related clinical conditions.
In the same MMWR, CDC adds three new conditions — pulmonary tuberculosis, recurrent pneumonia, and invasive cervical cancer — to the list of clinical indicators of AIDS. These new conditions mean that more women and injection drug users are expected be diagnosed with AIDS.
May 20, 1994
CDC Issues Guidelines for Organ and Tissue Transplants
The U.S. Centers for Disease Control and Prevention issues guidelines for preventing HIV transmission during organ and tissue transplants.
Learn More.
The guidelines follow a report to the CDC about a case of HIV transmission from a screened, antibody-negative donor to several transplant recipients.
Researchers Recommend AZT to Prevent Mother-to-Infant Transmission
The U.S. Public Health Service recommends that pregnant women be given the antiretroviral drug AZT to reduce the risk of perinatal transmission of HIV.
Learn More.
Following a workshop to develop recommendations for the use of AZT with HIV-infected women who are pregnant, the Public Health Service determines that AZT administered to a selected group of HIV-infected women and their infants is successful in reducing the risk of HIV transmission by approximately 66%.
In its report, the Public Health Service states that because the clinical status of many HIV-infected women may differ from that of the women in the trial, the recommendations should be tailored to each woman’s clinical situation.
“The potential benefits, unknown long-term effects, and gaps in knowledge about her specific clinical situation must be discussed with the woman,” the report states. “This information is intended to provide a basis for discussion between the woman and her healthcare provider so that the woman can weigh the risks and benefits of such therapy and make informed decisions about her treatment.”
December 23, 1994
FDA Approves Saliva HIV Test
The U.S. Food and Drug Administration approves an oral HIV test, the first non-blood-based antibody test for HIV.
Learn More.
FDA says the test, which uses fluid from the mouth instead of blood, will be available only from doctors and will be administered only by people trained to do so.
“As long as a positive test is followed up with a blood test and as long as there is appropriate counseling available, it is a reasonable thing to do,” Dr. Jeff Lawrence tells The New York Times. Dr. Lawrence is a consultant to the American Foundation for AIDS Research.
Studies show that for every 100 people infected with HIV, the oral-fluid-based test will miss one or two, and for every 100 people who are not infected, test results will be incorrectly positive for approximately two people.
July 7, 1995
U.S. Recommends HIV Testing for Pregnant Women
To address the increasing epidemic of HIV infection among women and their infants, the U.S. Public Health Service encourages pregnant women to voluntarily be tested for the virus.
Learn More.
Developed in collaboration with public health officials, service organization leaders and federal researchers, the recommendation for HIV testing stressed the importance of early diagnosis of infection for the health of both women and their infants.
In an edition of the Centers for Disease Control and Prevention’s MMWR, the results of a clinical trial are announced as a significant advance in HIV-related treatment and prevention. The placebo-controlled, clinical trial indicated that the administration of zidovudine to HIV-infected pregnant women and their newborns could reduce the risk for perinatal transmission of HIV by approximately 66%.
With this CDC-tested treatment, pregnant women who are HIV-positive could benefit from an early diagnosis.
HIV can be transmitted from an infected woman to her fetus or newborn during pregnancy, during labor and delivery, and during the postpartum period (through breastfeeding).
At the time, researchers had confirmed that transmission of HIV to a fetus could occur as early as the eighth week of gestation, but most perinatally transmitted infections occurred shortly before or during the birth process. The CDC estimated that breastfeeding could increase the rate of transmission by 10-20%.
In a 2003 interview with PBS News Hour, Dr. Mary Glenn Fowler, the lead CDC researcher on maternal-to-child HIV transmission, would credit the decline in babies being born with HIV to women following the CDC recommendation to get tested for HIV and the availability of the zidovudine treatment.
“It’s been one of our really strong successes in the HIV epidemic,” Dr. Fowler told PBS. “In the early ’90s we had approximately between 1,000 and 2,000 women delivering infected babies each year, and we have really reduced that [in 2003] down to close to 280 to 370 babies being infected. So it’s almost greater than an 80% decline, and it’s related to use of anti-retrovirals during pregnancy as well as to obstetrical intervention, such as scheduled C-section prior to the onset of labor.”
July 14, 1995
CDC Issues Guidelines on Prevention of Opportunistic Infections
The U.S. Centers for Disease Control and Prevention issue the first guidelines to help healthcare providers prevent opportunistic infections in people living with HIV.
Learn More.
In a precursor to a full report that would be published in the August edition of Clinical Infectious Diseases, the CDC announces that healthcare providers can prevent opportunistic infections in HIV-positive people by adhering to a set of guidelines.
The set of recommendations are rated according to the strength of the recommendation and the quality of evidence supporting the recommendation. The guidelines address prevention techniques for adults, adolescents and children.
The Centers for Disease Control and Prevention endorses a National Academy of Sciences report that concludes needle-cxchange programs are an effective method of preventing HIV infection.
Learn More.
In its review of Syringe Exchange Programs — United States, 1994-1995, a report by the National Academy of Sciences. the CDC expresses support for needle-exchange programs, stating that they are effective in reducing HIV transmission associated with drug injection.
The report states that as of December 1994, 35.3% of the 435,319 cases of AIDS reported among adults are associated with IV drug use. In addition, injection of illegal drugs is the risk behavior most frequently associated with heterosexual and perinatal transmission of HIV in the U.S.
The goal of needle-exchange programs is to reduce HIV transmission associated with IV drug use by providing sterile syringes in exchange for used, potentially HIV-contaminated syringes.
October 31, 1995
More than 500,000 AIDS Cases Reported to CDC
The number of AIDS cases exceeds 500,000 in the U.S., with 311,381 (62%) of them representing deaths.
Learn More.
In the CDC’sMorbidity and Mortality Weekly Report, the total number of persons in the U.S. reported to have AIDS climbs to 501,310.
According to the report, the rates per 100,000 population for reported AIDS cases in 1994 are:
48 in the Northeast,
31 in the South,
29 in the West, and
13 in the Midwest
However, during 1988-1992 and 1993-October 1995, the largest numbers of cases (65,926 and 86,462, respectively) were reported from the South, which also accounted for the largest proportionate increase of reported cases (31%).
December 7, 1995
FDA Approves First Protease Inhibitor
The U.S. Food and Drug Administration approves the first of a new class of drugs — protease inhibitors — designed to attack the HIV virus. This ushers in a new era of highly active antiretroviral therapy (HAART), which has the potential to extend life expectancies for people living with HIV.
Learn More.
The drug, saquinavir, manufactured by Hoffmann-La Roche, is a member of the new class of drugs called protease inhibitors that attack the ability of the HIV virus to reproduce. It does so by inhibiting an enzyme called protease that is crucial to HIV reproduction.
The first antiretroviral therapies developed for people with HIV are nucleoside reverse-transcriptase inhibitors (NRTIs), but these drugs would prove to be only partially effective. The addition of an orally administered protease inhibitor reduces HIV plasma concentrations and increases T-cell (CD4+) counts to levels that enable patients to have fairly normal life expectancies.
This combination — two nucleoside analogs and a protease inhibitor — is now considered the cornerstone of active antiretroviral therapy.
July 7, 1996
Conference Attendees Optimistic about HAART Treatment
The 11th International AIDS Conference in Vancouver highlights the effectiveness of highly active antiretroviral therapy (HAART), creating a period of optimism.
Learn More.
The first international AIDS conference in two years, the event is one of the more eagerly anticipated scientific meetings in years. Data on promising new drug treatments for AIDS, insights into the ways HIV infects cells, and the mechanisms of “host resistance” to that attack are scheduled to top the agenda.
Remarkable gains in using combinations of costly new and old drugs promise to slow the progression of AIDS and to allow many people infected with HIV to live longer and healthier lives, conference presenters announce to attendees.
With 15,000 delegates, journalists and commercial exhibitors in attendance, it is the largest conference so far. The theme is “One World, One Hope.”
While it seems that AIDS may finally become a managable disease in developed countries, less developed nations are struggling to scrape together the resources to provide necessary treatment and services to people with HIV and AIDS.
Data would be released at the conference that estimate a total of 21.8 million people to be currently living with HIV/AIDS, the vast majority of whom live in developing countries.
December 30, 1996
Researcher David Ho Develops ‘Hit Early, Hit Hard’ Treatment
HIV/AIDS researcher Dr. David Ho is named TIME magazine “Man of the Year” for advocating a new strategy for treating HIV – “hit early, hit hard.”
“We set up several studies in mid-1995, and by mid-1996 we were able to show that for the first time we could drop the virus down so that it’s not detectable and keep it down for a year or more,” Dr. Ho tells Frontline in a series of interviews in 2005-2006. “That was what was later hailed as the major advance in HIV therapeutics.”
1996
Total of U.S. AIDS Cases Begins to Decline
The number of new AIDS cases diagnosed in the U.S. declines for the first time since the beginning of the epidemic.
Learn More.
Ending the 16-year incline of cases, 1996 data shows that AIDS-related deaths dropped 23% from 1995 to 1996.
Experts credit the downturn with the availability of aggressive new therapies that keep infected patients healthier, as well as the possibility that fewer people are becoming infected in the first place.
African-American women are particularly at risk. In 1994, officials at the Centers for Disease Control reported that black women were almost 15 times as likely as white women to test positive for HIV.
”My new cases among women are often young women, coming in with a first pregnancy who are being tested as part of that pregnancy and finding out that they are HIV-positive,” said Dr. Mary Young, who treats AIDS patients at Georgetown University here.
“The gay community has done a wonderful job of getting the message out. But I don’t know that we target young African-American women very well.”
September 26, 1997
FDA Approves First Antiretroviral Drug Combo
The U.S. Food and Drug Administration approves Combivir, the first one-pill combination of the two most widely used antiretroviral medications for AIDS and HIV infection.
As the first combination agent, the medication significantly simplies HIV therapy. Combivir becomes the gold standard nucleoside “backbone” until the mid-2000s, when the introduction of newer fixed-dose combinations with improved tolerability and toxicity arrive.
December 1997
Protease Inhibitor Use Leads to Drug Resistance in Some
As a greater number of people begin taking protease inhibitors, resistance to the drugs becomes more common, and drug resistance emerges as an area of grave concern within the AIDS community.
Sub-Saharan Africa Shows More Women Infected than Men
In June, UNAIDS reports that the number of women living with HIV/AIDS in sub-Saharan Africa now exceeds that of men.
September 2, 1998
AIDS Researchers Die in Plane Crash
Jonathan Max Mann, M.D., known as the “architect of the global mobilization against AIDS,” and his wife, Mary Lou Clements-Mann, M.D. of Johns Hopkins University, are among the 229 people who die in the crash of Swissair Flight 111. The couple were traveling to an HIV vaccine meeting in Geneva.
Learn More.
Dr. Mann, 51, was world-renown for his role as the founding director of the World Health Organization’s Global Program on AIDS He had recently become dean of Allegheny University of the Health Sciences’ School of Public Health in Philadelphia.
Dr. Clements-Mann of Johns Hopkins University, also 51, was a distinguished researcher in vaccine development at Johns Hopkins University.
“This is shocking,” Dr. Anthony Fauci, director of NIAID, said to the Los Angeles Times. “We’ve lost two fine human beings, as well as two major contributors to the AIDS effort who were there from the very beginning.”
The couple often travelled to Geneva, the headquarters of WHO and site of numerous international scientific meetings on AIDS. The regular Swissair flight out of New York to Geneva was considered by many as “a U.N. airbus,” because so many U.N. agencies were based in Geneva.
Also dying in the plane crash were Klaus Kinder-Geiger, a researcher at Brookhaven National Laboratory; Per Spanne, also Brookhaven researcher; Roger Williams, a cardiovascular geneticist at the University of Utah; and several staff members from the United Nations.
As the first director of the U.N. World Health Organization (WHO) campaign against AIDS, Dr. Mann was known world over for his early efforts to combat AIDS. Hailed as a human rights leader, he traveled to scores of nations to bring global and political attention to the seriousness of the epidemic.
“I was struck at the time that he looked much more beyond the research. He was very interested in the political implications of the epidemic. He was already convinced that AIDS would have broad social implications,” said Peter Piot, who worked with Dr. Mann in Zaire in 1984. “He changed my vision and view on all this.”
One of the world’s foremost authorities on global AIDS, Dr. Mann co-wrote two books defining and analyzing the global epidemic. Although his background was in medicine and not law, he contributed significant work to many law-related publications on the subject of human rights and healthcare.
In a 1996 essay for The John Marshall Law Review titled “Human Rights and AIDS: The Future of the Pandemic,” Dr. Mann argued that general principles of international human rights law, and specifically those grounded in the Universal Declaration of Human Rights, should guide medical personnel, public health policy makers, and governments in their responses to HIV and AIDS.
“His article reflected a global vision that the only appropriate responses to the HIV and AIDS pandemic would link human rights to public health,” wrote Mark E. Wojcik, a law professor at The John Marshall Law School in Chicago, in his tribute to Dr. Mann.
As the director of WHO’s campaign against AIDS from 1986 to 1990, Dr. Mann founded the United Nations’ Special Programme on AIDS on the principle that international cooperation was essential to combat the disease.
“Assurance of global collaboration is of the highest priority,” Dr. Mann said at the time, “for AIDS cannot be stopped in any country until it is stopped in all countries.”
Under Dr. Mann, the UN’s HIV/AIDS program (later renamed the Global Programme on AIDS) developed evidence that the only effective responses to HIV were those that respected the human rights of persons affected by the disease, according to Professor Wojcik.
“This stance influenced subsequent declarations on AIDS by focusing not only on the need for international cooperation, but on the protection of human rights as a fundamental public health strategy,” wrote Wojcik in 1998 for the UIC Law Review. “Mann’s advocacy for the protection of human rights as a key to public health also came in severe contrast to the positions of some governments and public health officials, who argued that the only effective response to AIDS was to imprison or deport persons with the virus.”
Dr. Mann received constant resistance to his humane approach to HIV/AIDS care, some times from within the UN system, and this led him to resign from WHO in protest in 1990.
His wife, Dr. Clements-Mann, was remembered by colleagues as a tireless advocate for vaccines, according to The Washington Post. She was working on a vaccine for HIV infection at the time of her death.
“In designing and conducting clinical trials for vaccines, she was as good as anyone in the world,” said Donald Burke, the director of the Center for Immunization Research at the school.
In 1999, the CDC Foundation would create the Jonathan M. Mann Memorial Lecture Fund in honor the late AIDS advocacy pioneer. The grant supports the annual Jonathan M. Mann Memorial Lecture, which is administered by the Council of State and Territorial Epidemiologists during its annual conference. The CDC Foundation is a nonprofit which supports the Centers for Disease Control and Prevention’s critical health protection work.
Also in 1999, the Mary Lou Clements-Mann Memorial Lecture in Vaccine Sciences would be created by National Foundation for Infectious Diseases to honor the vaccinologist and her work. The lecture is presented each year at the NFID Annual Conference on Vaccinology Research.
March 1999
U.S. Firm Begins Human Trials for Vaccine in Thailand
VaxGen, a San Francisco-based biotechnology company, begins conducting the first human vaccine trials in Thailand.
December 10, 1999
CDC Updates HIV Definition to Help Extend State Reach
he U.S. Centers for Disease Control and Prevention releases a new HIV case definition to help state health departments expand their HIV surveillance efforts and more accurately track the changing course of the epidemic.
July 2002
HIV/AIDS Tops Causes of Death in Sub-Saharan Africa
UNAIDS (the Joint United Nations Programme on AIDS) reports that HIV/AIDS is now by far the leading cause of death in sub-Saharan Africa, and the fourth biggest global killer. Average life expectancy in sub-Saharan Africa falls from 62 years to 47 years as a result of AIDS.
July 2002
Dozens of Countries Suffer from HIV/AIDS Spread
The 14th International AIDS Conference is held in Barcelona, Spain from July 7-12. Dozens of countries report they are experiencing serious HIV/AIDS epidemics, and many more are on the brink.
2002
10 Million People Aged 15-24, Worldwide, Live With HIV
Worldwide, 10 million young people, aged 15-24, and almost 3 million children under 15 are living with HIV. During this year, approximately 3.5 million new infections will occur in sub-Saharan Africa, and the epidemic will claim the lives of an estimated 2.4 million Africans.
2002
Side Effects, Drug Resistance Call Therapy Strategy Into Question
Side effects and increasing evidence of drug resistance call into question the “hit early, hit hard” strategy.
November 7, 2002
FDA Approves New Rapid-Diagnosis Test
The U.S. Food and Drug Administration announces the approval of the OraQuick Rapid HIV-1 Antibody Test with 99.6% accuracy. A second FDA-approved rapid HIV test, Single Use Diagnostic System for HIV-1, remains available.
Learn More.
Unlike other antibody tests for HIV, this blood test can be stored at room temperature, requires no specialized equipment, and may be used outside of traditional laboratory or clinical settings, allowing more widespread use of HIV testing.
The new test provides a result in about 20 minutes, while the fastest test currently in use takes 90 minutes. In practice, however, most people who seek AIDS testing aren’t given their results for a week or more after they provide a blood sample.
The OraQuick Test requires that a person prick his finger and use a wire loop to capture a drop of blood. The drop is then put in a vial containing a diluting solution.
Then a paper tab attached to a cap is lowered into the solution. A dark line appears on the tab if it makes contact with certain universal blood proteins. If antibodies to HIV are present, a second dark line appears.
Public health officials are hopeful that the test will substantially increase the number of people seeking testing, and decrease the fraction who, once tested, never return for the results.
February 24, 2003
Early AIDS Vaccine Trial Fails
VaxGen, a San Francisco-based biotechnology company, announces that its AIDSVAX vaccine trial failed to reduce overall HIV infection rates among those who were vaccinated.
March 31, 2003
Gates Foundation Donates $60 Million to HIV Research
The Bill and Melinda Gates Foundation awards a $60 million grant to the International Partnership for Microbicides to support research and development of microbicides to prevent transmission of HIV.
2003
Majority of New U.S. Infections Come from Lack of Knowledge
The U.S. Centers for Disease Control and Prevention (CDC) calculate that 27,000 of the estimated 40,000 new infections that occur each year in the U.S. result from transmission by individuals who do not know they are infected.
March 26, 2004
Diagnostic Test Based on Oral Fluid Samples Approved
The U.S. Food and Drug Administration (FDA) approves the use of oral fluid samples with a rapid HIV diagnostic test kit that provides the result in approximately 20 minutes.
January 26, 2005
700,000 in Developing Countries Receive Antiretroviral Therapies
The World Health Organization (WHO), UNAIDS (the Joint United Nations Programme on HIV/AIDS) , the U.S. Government, and the Global Fund to Fight AIDS, Tuberculosis, and Malaria announce results of joint efforts to increase the availability of antiretroviral drugs in developing countries. An estimated 700,000 people have been reached by the end of 2004.
September 22, 2006
CDC Revises Guidelines on HIV Testing
The U.S. Centers for Disease Control and Prevention (CDC) release revised HIV testing recommendations for healthcare settings, recommending routine HIV screening for all adults, aged 13-64, and yearly screening for those at high risk.
December 2006
Study Indicates Medical Circumcision Reduces Risk for HIV
A study of Kenyan men suggests that medical circumcision reduces by 53% their risk of acquiring HIV during heterosexual intercourse.
Learn More.
Conducted by the University of Illinois at Chicago and supported by the U.S. National Institute for Allergy and Infectious Diseases and the Canadian Institute of Health Research, the analysis of the clinical trial confirmed the importance of established risk factors for HIV and identified practices (such as circumcision) that warrant further investigation.
The study’s researchers said their goal was to “determine whether male circumcision had a protective effect against HIV infection, and to assess safety and changes in sexual behaviour related to this intervention.”
After compiling data from 2,784 men aged 18-24 years in Kisumu, Kenya, the researchers concluded that male circumcision significantly reduces the risk of HIV acquisition in young men in Africa.
“Where appropriate, voluntary, safe, and affordable, circumcision services should be integrated with other HIV preventive interventions and provided as expeditiously as possible,” the report stated.
2007
Over 565,000 U.S. Deaths From AIDS
CDC reports over 565,000 people have died of AIDS in the U.S. since 1981.
August 6, 2008
CDC Corrects Undercount of New HIV Cases
The U.S. Centers for Disease Control and Prevention release new U.S. HIV data showing a substantially higher infection rate than it previously estimated.
Learn More.
The CDC’s new report adjusts the previous number of new infections per year from 40,000 to 56,300.
The adjusted data did not represent an actual increase in the numbers of HIV infections, explained the CDC; instead, the data reflected a more accurate way of measuring new infections. A separate analysis suggested that the annual number of new infections was never as low as 40,000 and that the rate of new infections was stable since the late 1990s.
October 6, 2008
Nobel Prize Awarded for 1983 Discovery of HIV
The Nobel Prize in medicine is awarded to two French virologists, Françoise Barré-Sinoussi, and Luc A. Montagnier, for their 1983 discovery of HIV, the virus that causes AIDS.
February 2009
Washington DC Reports HIV Rate Higher than West Africa
Washington, DC has a higher rate of HIV (3% prevalence) than West Africa– enough to be a “severe and generalized epidemic.”
Learn More.
According to a report issued by the District of Columbia, the HIV rate in the nation’s capital is the highest in the country with nearly 3% of residents living with HIV or AIDS.
“That’s a little more than 15,000 people with the disease — a total that well exceeds the 1% threshold for what makes up a ‘generalized and severe epidemic,'” stated news coverage from NBC‘s Washington station.
The study found that every form of transmission is on the rise, with minorities and women at an especially high risk. The rate among heterosexual black women was 15 times more than the rate of white women and more than three times that of Latinas.
Patricia Nalls, Founder and Executive Director of The Women’s Collective, told NPR, “Women and girls are at risk for several reasons. Prevention messages are not addressing women’s needs. And you are not seeing women in the face of the campaigns and the messages that’s out there.”
Nalls said that violence against women also needs to be considered when addressing HIV infection among the female population. She urged the local government to declare a state of emergency.
October 6, 2009
100th Antiretroviral Drug Approved
The U.S. Food and Drug Administration approves the 100th antiretroviral drug.
Learn More.
FDA announces that it has approved the 100th antiretroviral drug under the President’s Emergency Plan for AIDS Relief (PEPFAR). Of the more than 100 products that have received either full or tentative FDA approval under the program, 29 are branded drugs and 71 are generics.
The FDA process was launched in May 2004, in response to a call from activists, clinicians and members of Congress to use the WHO’s pre-certification drug list to make purchases of generic medications for PEPFAR-funded programs. Instead, a process was devised to allow the FDA to certify generic antiretrovirals (ARVs) for PEPFAR purchase, even if the branded drug was still protected by U.S. patent laws.
HHS Secretary Kathleen Sebelius said in a statement, “This milestone exemplifies the dedication, caring, and hard work of all who strive to better the lives of those infected with or affected by HIV/AIDS.”
2010
iPrEx Study Shows Risk Reduction in HIV-Negative Men
A new study shows that a daily dose of HIV drugs reduced the risk of HIV infection by 44% among HIV-negative men who have sex with men.
Learn More.
The National Institutes of Health announce these results from its iPrEx study, supporting the concept of pre-exposure prophylaxis (PrEP) in a targeted population.
August 27, 2010
Origin of HIV-1 Traceable to Chimpanzees in Africa
Research scientists chart the origin of AIDS to wild-living chimpanzees infected with simian immunodeficiency viruses (SIVs).
Learn More.
In an article published in the scientific journal Philosophical Transactions B titled “The Evolution of HIV-1 and the Origin of AIDS,” researchers Paul M. Sharp and Beatrice H. Hahn demonstrated that HIV-1 can be traced via evolutionary comparisons to SIV-infected chimps and gorillas in west central Africa.
Sharp and Hahn described in their paper the four lineages of HIV-1 that resulted from cross-species transmissions from chimps (and possibly gorillas) to humans. Their research was supported by grants from National Institutes of Health and the Bristol Myers Freedom to Discover program.
“The conclusion that HIV-1 was derived from a virus infecting chimpanzees is particularly interesting, because chimpanzees and humans are so closely related,” Sharp and Hahn wrote. “This raises a number of questions, such as the origin of the chimpanzee virus, whether adaptation of SIVcpz to infecting chimpanzees rendered the virus more capable of infecting humans and whether SIVcpz infection of chimpanzees is pathogenic.”
In the January 2000 article “AIDS as a Zoonosis: Scientific and Public Health Implications,” Sharp, Hahn and two additional researchers theorized how the virus was able to be transmitted from chimpanzees to humans. Since transmission requires “exposure to infected blood and body fluids,” they propose that it was likely that infection in humans occurred during the practice of hunting and butchering chimps. Even though the opportunity for chimp-to-human transmission existed for hundreds of years, the Congo in the early 20th Century, then under colonization by the Dutch, had a set of circumstances that for the first time allowed the virus to spread from humans to other humans.
Since workers in the bushmeat industry usually operated in a remote area in the southeast corner of Cameroon, Sharp and Hahn were able to identify this region as the likely location of the first notable spread of the disease. Around 1920, HIV infections occurred in humans in “at least a dozen independent transmissions” from chimps. From there, these infected people spread the virus as they travelled by the Sangha River to the largest city to the south, the Congolese capital city of Kinshasa (which was then under Dutch colonization).
“During the early part of that century, the destabilization of social structures by invading colonial powers, the origin and rapid growth of major conurbations, and the widespread use of injections may all have contributed to provide an unprecedented opportunity for dissemination of blood-borne viruses,” Sharp and Hahn wrote.
In October 2018, historian Thomas F. McDow would reference much of Sharp and Hahn’s research in an article for Origins delving into how the spread of HIV was linked to the socio-political impact from Africa’s colonization and the globalization of the economy in the early 20th century.
In “A Century of HIV,” McDow wrote: “The story of HIV is a story of globalization. The expanding connections of the 20th Century spread the disease, yet the limitations and inequalities of global public health allowed the disease to ravage populations even after scientists discovered effective drug treatments.”
McDow credited research scientists with being able to pinpoint the origin of HIV from blood samples and a lymph node dating back to the late 1950s and stored in a Congolese laboratory.
“This virus began its career in humans at a time when the forests and riverine landscapes of Equatorial Africa became increasingly connected to the global economy,” McDow wrote. “While the people who lived in these forests had traded and been connected to wider regional networks for a very long time, the scope and scale of these interactions changed at the end of the nineteenth and beginning of the twentieth centuries.”
In 1884, major European nations convened the Berlin Conference (also known as the Congo Conference), and determined which countries would control the trade routes in Central Africa, according to McDow. Eight of the 14 countries represented at the conference — Germany, Belgium, Spain, France, the United Kingdom, Italy, Portugal, and the Ottoman Empire — set about laying claim to various African territories.
Under the control of European companies, the Sangha river basin became the world’s main producer of ivory and rubber. To support their industry, the European colonists modernized the infrastructure of their territories and built links to previously unconnected regions. Two towns on opposite sides of the Congo River, Kinshasa and Brazzaville, attracted Africans from remote parts of the continent with the promise of work and wages.
Meanwhile, Africans continued to live in impoverished conditions and workers were brutally exploited for decades, according to McDow. As indigenous African workers began to rebel and refuse to accept to be treated poorly by the colonists, more wealth and opportunity began to come their way — but just a little.
“In the 1940s and 1950s, the creative energies of these towns produced the lively sounds of rumba, music inspired in part by Latin American sound and driven by the distinctive Congolese guitar playing,” wrote McDow. “But the same venues and impulses that attracted the youth to hear people like Wendo Kolosoy croon ‘Marie Louise’ created conditions for the spread of the virus through heterosexual intercourse.”
During this time, records showing the uptick in sexually transmitted diseases like Hepatitis B suggests that HIV was also likely spreading during this time. Then came the 1960s, a time hailed as “The African Decade” when people in the colonized territories fought for and won their independence.
The United Nations Education, Science, and Cultural Organization (UNESCO) and the Congolese government responded the region’s lack of skilled workers among its indigenous people by recruiting teachers and doctors to work in the Congo, according to McDow. Belgians and Haitians made up the largest groups of expatriate professionals.
“While in Congo, however, some contracted HIV and subsequently returned home with the deadly, unknown virus,” he wrote. “The earliest cases of HIV in the United States are connected to Haiti, and the Haitian-Congo link seems to have helped the disease cross the Atlantic.”
All of these events leading up to the June 1981 Morbidity and Mortality Weekly Report by The Centers for Disease Control are the “pre-history of AIDS,” according to McDow.
“Looking back, doctors can see that a small number of unexplained medical cases in the west … were early cases of AIDS,” wrote McDow.
Among these early cases are:
In 1939-1959, cases of Pneumocystis pneumonia were reported in Western Europe in infants born prematurely. Researchers state that the most likely cause was a retrovirus closely related to HIV (or a mild version of HIV) brought to Europe and originating from Cameroon, a former German colony. The epidemic started in 1939 along the German-Polish border in the Free City of Danzig and then spread to nearby countries, like Germany, Switzerland and The Netherlands, in the 1940s and 1950s.
On June 28, 1959, Antonio Ardouin, a 49-year-old Jamaican-American shipping clerk, died in New York City of Pneumocystis carinii pneumonia. Gordon Hennigar, who performed the postmortem examination of the man’s body, found the case to be so unusual, he preserved Ardouin’s lungs for later study. Hennigar has been quoted as saying that he believes Ardouin likely died of AIDS.
On May 15, 1969, Robert Rayford, a 15-year-old Black youth, died at St. Louis City Hospital with no immune system to fight the infection that ravaged his body for more than a year. An autopsy revealed widespread Kaposi’s sarcoma, and a 1988 test of autopsy tissue specimens showed evidence of nine distinct HIV proteins.
In 1976, Arvid Noe, a Norwegian sailor, died; it was later determined that he contracted HIV/AIDS in Africa during the early 1960s. His wife and daughter also died of AIDS-related illnesses.
On June 28, 1978, a Portuguese man known as Senhor José (“Mr. Joseph”) died. Later confirmed as the first known infection of HIV-2, he was believed to have been exposed to the disease in Guinea-Bissau in 1966.
In 1978-79, eight people from New York and San Francisco participated in a Hepatitis B virus study, and about 40 years later, their reconstructed blood samples tested positive for HIV. A 2016 re-testing of samples from the Hep B studies identified five HIV cases from New York and three from San Francisco. From their data, researchers estimate the virus’ entry into the U.S. at about 1970. “You see a very telltale pattern of extensive genetic diversity in New York City, suggesting that New York City was the key hub of diversification for the virus,” researcher Michael Worobey told PBS News Hour in 2016. ““Restricted genetic diversity in San Francisco, suggesting San Francisco was a later dispersal out of this New York City hub.”
In 1979, a five-year-old girl died in New Jersey after suffering from symptoms of AIDS since birth; later her stored tissues tested positive for HIV-1. The girl’s mother was described as an intravenous-drug user who had multiple male sex partners.
On December 24, 1980, Rick Wellikoff, a Brooklyn grade-school teacher, died at the age of 37 of various infections that overwhelmed his immune system. Strong evidence suggests that he died of AIDS.
On January 15, 1981, Nick Rock, a New York City bartender and friend of Rick Wellikoff, died after months of suffering from seizures, heart attacks and Kaposi’s sarcoma.
April 11, 2011
Public Debates Transplant Ban of HIV-Infected Organs
Public debate begins on whether the longstanding ban on transplants of HIV-infected organs should be dropped .
July 13, 2011
CDC Study Supports Use of PrEP As Preventative Therapy
A new CDC study and a separate clinical trial (the Partners PrEP study) provide the first evidence that adaily oral dose of antiretroviral drugs used to treat HIV infection can also prevent new infections in individuals exposed to HIV through heterosexual sex.
July 17, 2011
Studies Confirm Efficacy of Antiretroviral Therapies
Scientists announce that two studies have confirmed that daily antiretroviral drugs can significantly lower the rates of HIV-related infection.
Learn More.
The announcement is made at the International AIDS Society’s Conference on HIV Pathogenesis, Treatment, and Prevention in Rome on July 17-20. The studies show that individuals taking daily antiretroviral drugs experienced infection rates more than 60% lower than those on a placebo.
September 27, 2011
‘Origins of AIDS’ Traces Disease Back to Early 1900s Africa
The book The Origin of AIDS by Canadian researcher Jacques Pépin chronicles the emergence of HIV/AIDs in Africa in the early part of the 20th Century and its evolution into a global pandemic.
Learn More.
Dr. Pépin, an epidemiologist and HIV/AIDS expert based in Quebec, traced the AIDS virus back to a single bush hunter in Central Africa in 1921. He used medical reports and technical data dating back to France’s colonization of African territories to piece together the beginnings of a disease that would eventually leap from continent to continent and kill more than 40 million people worldwide.
“Either a hunter got injured with his knife when he cut out the ape to bring the carcass back to the village so that the chimp’s blood became in contact with his own blood, or the same type of accident occurred during the actual cooking of chimpanzee meat,” he said in an interview with Cambridge University Press, the publisher of his book.
“Three other potential modes of transmission from chimp to man, which have been proposed over the years, can now be rejected,” he added, “since there is nothing to sustain these other hypotheses.”
“On my first day there, to my amazement, I suddenly understood, while looking at the health systems annual reports, the scope of the colonial-era public health interventions that required the administration of massive amounts of IV drugs over the whole of central Africa and throughout several decades,” he said.
Dr. Pépin told Cardwell it took four years to research and write The Origin of AIDS, and an additional year to edit the manuscript with the publisher.
“The book sheds new light on the pivotal role French colonialism played in spreading HIV from likely a single bush hunter infected with a simian immunodeficiency virus in central Africa in the early 1920s to large swaths of Africa and beyond,” Cardwell wrote in his 2012 article “The Story of the Origins of AIDS.”
Dr. Pépin’s book describes the conditions in turn-of-the-century French West Africa that created the ideal petri dish for a new disease.
At the Berlin Conference of 1884-1885, France was one of several European countries to lay claim to colonial territories in Africa. In the decades to come, the urbanization of central Africa, inferior health policies, and the rise of prostitution all led first to the persistence of HIV in the population in the 1930s-1950s, and then eventually to its spread.
After about 50 years of managing an enterprise that involved extracting the area’s natural resources while ruling over its indigenous peoples, the French introduced a medical program in the 1930s that routinely used unsterilized syringes and employed other shoddy practices in the treatment of tropical diseases. Dr. Pépin contended that these were the conditions in which HIV was able to take hold and then propagate.
In The Origins of AIDS, Dr. Pépin also explained how the construction of a railroad line across the African jungle resulted in the creation of sprawling government-run camps that were unsanitary and dangerous. Among the camp residents, according to Dr. Pépin, were health-compromised workers and prostitutes from across the colonial territories.
Dr. Pépin said he took research results from molecular biologists working under Beatrice H. Hahn, M.D. and scientists led by Michael Worobey, M.D., and used this to inform his own research drawn from colonial archives and European libraries.
“I conducted epidemiological studies which documented that several blood-borne viruses were indeed transmitted during several medical interventions in different parts of Africa,” Dr. Pépin said.
Dr. Pépin started his career in the early 1980s as a medical officer in a Zaire bush hospital. After returning to Canada to complete his education in medicine, he returned to Africa as a clinical researcher at the Medical Research Council Laboratories in a tiny West African country called The Gambia. This is where he began researching HIV and its interaction with sexually transmitted diseases.
“In the course of my investigations, I met most of the few hundred Senegalese prostitutes who charged their Gambian brothers rock-bottom prices for a few moments of pleasure,” Dr. Pépin wrote in the forward of the 2021 edition of The Origins of AIDS.
November 20, 2011
Rate of Global Infections & Deaths Level Off
New data shows global HIV prevalence is much lower than previously believed (33 million cases instead of 40 million).
The data also indicates a decline in the numbers of new infections and people dying from AIDS-related illnesses, due in part to HIV-prevention programs and antiretroviral therapy.
The report also announces that, for the first time, the prospect of a microbicide that contains antiretroviral medicine is providing additional hope to the women in sub-Saharan Africa, who continue to bear a disproportionate burden of the HIV epidemic in this region.
Days later, the Obama administration announces new goals for PEPFAR (the President’s Emergency Plan for AIDS Relief), saying it is “the beginning of the end of AIDS.”
“Today is a remarkable day,” President Barack Obama says in a White House statement. “Today, we come together, as a global community, across continents, faiths and cultures, to renew our commitment to ending the AIDS pandemic – once and for all.”
December 23, 2011
Science Journal Announces ‘Breakthrough of the Year’
The journal Science announces that it has chosen the HPTN 052 study as its 2011 Breakthrough of the Year.
March 13, 2012
Researchers Link ART Therapy to Cardiovascular Disease
A new study suggests that people living with HIV and taking antiretroviral therapy (ART) have an increased risk of cardiovascular disease.
Learn More.
Researchers from the University of New South Wales in Australia release the results of a study that show that people living with HIV who are taking antiretroviral therapy (ART) have an increased risk of cardiovascular disease.
“Although the health and survival of PLHIV have improved with effective ARTs, people living with HIV are at substantially greater risk of developing other comorbidities, such as cardiovascular disease, compared with uninfected people,” the researchers conclude.
Due to the prevelance of cardiovascular disease and its cause of deaths worldwide, this poses a significant issue for people living with HIV, particularly as they get older, according to the researchers.
July 3, 2012
FDA Approves First At-Home Test
The FDA approves the first at-home HIV test that will let users learn their HIV status right away.
July 16, 2012
Truvada for PrEP Approved
The FDA approves the use of Truvada® for pre-exposure prophylaxis (PrEP). Adults who do not have HIV, but who are at risk for infection, can now take this medication to reduce their risk of getting the virus through sexual activity.
March 4, 2013
Case Reported of HIV-Infected Child ‘Functionally Cured’
NIH-funded scientists announce the first well-documented case of an HIV-infected child, designated as “the Mississippi Baby,” who appears to have been functionally cured of HIV infection (i.e., no detectable levels of virus or signs of disease, even without antiretroviral therapy.
June 2, 2013
NY Times Addresses Middle-Aged People Living With HIV
The New York Times runs two articles which focus on middle-aged people living with HIV: The Faces of H.I.V. in New York in 2013 and ‘People Think It’s Over’: Spared Death, Aging People With H.I.V. Struggle to Live
June 5, 2013
NMAC Issues Plan on Mitigating the Impact of HIV on Black Men
The National Minority AIDS Council (NMAC) releases RISE Proud: Combating HIV Among Black Gay and Bisexual Men, an action plan to mitigate the impact of HIV on black gay and bisexual men.
July 2, 2013
Bone Marrow Transplant Recipients Reportedly Cured of HIV
Researchers report that two HIV-positive patients in Boston who had bone-marrow transplants for blood cancers have apparently been virus-free for weeks since their antiretroviral drugs were stopped
December 31, 2013
UNAIDS: Steep Drop in HIV in Low-to-Middle Income Countries
UNAIDS announces that new HIV infections have dropped more than 50% in 25 low- and middle-income countries, and the number of people getting antiretroviral treatment has increased 63% in the past two years.
January 2, 2014
‘Cured’ HIV Cancer Patients Relapse
News sources report that the two Boston patients believed to have been cured of HIV after undergoing treatment for cancer have relapsed
February 3, 2014
amfAR Launches $100 Million Research Initiative
amfAR announces the launch of Countdown to a Cure for AIDS, a $100 million research initiative aimed at finding a broadly applicable cure for HIV by 2020.
March 4, 2014
Initial Research Supports ‘Undetectable = Untransmittable’ Concept
European researchers announce the results of the first phase of the PARTNER Study, an observational study focusing on the risk of sexual HIV transmission when an HIV-positive person is on treatment.
Learn More.
The study found that no HIV-positive partner who was undergoing antiretroviral therapy and had an undetectable viral load had transmitted HIV.
July 10, 2014
‘Mississippi Baby’ No Longer Undetectable
The National Institutes of Health announce that the “Mississippi baby” now has detectable levels of HIV after more than two years of showing no evidence of the virus.
September 9, 2014
Southern States Become New U.S. Epicenter of HIV
The Pew Charitable Trust publishes Southern States Are Now Epicenter of HIV/AIDS in the U.S.
October 3, 2014
Pre-History of HIV Traced to Congo in Science Magazine Report
Researchers publish an article in Science that charts the spread of HIV from its origins in early 20th Century chimpanzee hunters in the Cameroon to its eventual transmission to residents of Kinshasa, the capital of the Democratic Republic of the Congo.
Learn More.
Using statistical approaches applied to HIV-1 sequence data from central Africa, the international team of researchers showed that from the 1920s, Kinshasa (formerly known as the Dutch-colonized city Leopoldstad) was the site of early HIV transmission. The researchers validated their location and dating estimates by using the earliest HIV-1 archival sample, also from Kinshasa.
From Kinshasa, the virus spread in the early 1960s to other areas of the Congo via rail links, according to the report titled “The early spread and epidemic ignition of HIV-1 in human populations.” HIV then spread from Africa to Haiti when Haitian teachers, brought to the Congo in the 1960s and 1970s to assist with Congolese independence, returned home.
An estimated 4,500 Haitians were in the Congo in the 1960s, and that number grew in the 1970s, according to Thomas F. McDow, a historian of Africa and the Indian World at the Ohio State University. .
Only 30% of HIV-Positive People Have ‘Virus Under Control’
CDC announces that only 30% of Americans with HIV had the virus under control in 2011, and approximately two-thirds of those whose virus was out of control had been diagnosed but were no longer in care.
January 8, 2015
Injectable Contraceptive May Increase Women’s Risk of HIV
A review of multiple studies of South African women indicates that using Depo Provera, an injectable contraceptive, may increase women’s chances of contracting HIV by 40 percent.
February 23, 2015
CDC: More Than 90% of New Infections Preventable
CDC announces that more than 90% of new HIV infections in the U.S could be prevented by diagnosing people living with HIV and ensuring they receive prompt, ongoing care and treatment.
Learn More.
Published by the CDC and subsequently in JAMA, the American Medical Association’s journal, a report by Jacek Skarbinski, M.D., and Eli Rosenberg, M.D. announces that persons living with HIV who are retained in care and have achieved viral suppression are 94.0% less likely to transmit HIV than HIV-infected undiagnosed persons.
“Unfortunately, too few persons living with HIV have achieved viral suppression,” the report concludes. “These estimates of the relative number of transmissions from persons along the HIV care continuum highlight the community-wide prevention benefits of expanding HIV diagnosis and treatment in the United States.”
The report recommends the implementation of improvements at each step of the continuum to reduce HIV transmission.
“Through stronger coordination of efforts among individuals, HIV care providers, health departments, and government agencies, the United States can realize meaningful gains in the number of persons living with HIV who are aware of their status, linked to and retained in care, receiving ART, and adherent to treatment,” state the researchers.
February 25, 2015
HIV Outbreak in Indiana Tied to Injection Drug Use
Indiana state health officials announce an HIV outbreak linked to injection drug use in the southeastern portion of the state. By the end of the year, Indiana will confirm 184 new cases of HIV linked to the outbreak.
April 15, 2015
NIH Launches Study of Heart Disease Among HIV+
NIH launches a large, multicenter, international clinical trial to study heart disease in people living with HIV, who are up to twice as likely as HIV-negative individuals to have heart attacks and other forms of cardiovascular disease.
May 27, 2015
START Study Shows Reduced Risk of AIDS
Results from the Strategic Timing of AntiRetroviral Treatment (START) study indicate that HIV-positive individuals who start taking antiretroviral drugs before their CD4+ cell counts decrease have a considerably lower risk of developing AIDS or other serious illnesses.
Learn More.
Subsequent data releases show that early therapy for people living with HIV also prevents the onset of cancer, cardiovascular disease, and other non-AIDS-related diseases.
June 30, 2015
Cuba Eliminates Mother-to-Child HIV Transmission
The World Health Organization certifies that Cuba is the first nation to eliminate mother-to-child transmission of both HIV and syphilis.
July 20, 2015
Study Shows Effectiveness of Antiretrovirals in Preventing Transmission
Researchers report that antiretroviral therapy is highly effective at preventing sexual transmission of HIV from a person living with HIV to an uninfected heterosexual partner, when the HIV-positive partner is virally suppressed. The finding comes from the decade-long HPTN 052 clinical trial.
July 23, 2015
FDA Approves Test Differentiating Between HIV-1 & HIV-2
The U.S. Food and Drug Administration approves the first diagnostic test that differentiates between different types of HIV infections (HIV-1 and HIV-2). The test can also differentiate between acute and established HIV infections.
November 24, 2015
UNAIDS: Nearly 16 Million Accessing Retroviral Treatment
UNAIDS releases its 2015 World AIDS Day report which finds that 15.8 million people were accessing antiretroviral treatment as of June 2015—more than doubling the number of people who were on treatment in 2010.
December 6, 2015
HIV Diagnoses Drop 19% from 2005 to 2014
CDC announces that annual HIV diagnoses in the U.S. fell by 19% from 2005 to 2014. There were steep declines among heterosexuals, people who inject drugs, and African Americans (especially black women), but trends for gay/bisexual men varied by race/ethnicity.
Learn More.
Diagnoses among white gay/bisexual men decreased by 18%, but they continued to rise among Latino gay/bisexual men and were up 24%. Diagnoses among black gay/bisexual men also increased (22%), but the increase has leveled off since 2010.
January 19, 2016
Only 20% of Sexually Active High School Students Test for HIV
The U.S. Centers for Disease Control and Prevention report that only 1 in 5 sexually active high school students has been tested for HIV. An estimated 50% of young Americans who are living with HIV do not know they are infected.
January 28, 2016
Researchers Report Increasing Resistance to Tenofovir
Researchers announce that an international study of over 1,900 patients with HIV who failed to respond to the antiretroviral drug tenofovir—a key HIV treatment medication—indicates that HIV resistance to the medication is becoming increasingly common.
February 25, 2016
First Report of HIV Infection Despite Truvada
At the annual Conference on Retroviruses and Opportunistic Infections (CROI), researchers report that a man taking the HIV-prevention pill Truvada® has contracted HIV—marking the first reported infection of someone regularly taking the drug.
March 3, 2016
Researchers Report Gender Differences in Truvada Dosage
Pharmacy researchers report finding that women need daily doses of the antiviral medication Truvada® to prevent HIV infection, while men only need two doses per week due to differences in the way the drug accumulates in vaginal, cervical and rectal tissue.
May 12, 2016
NIH Announces HIV Vaccine Trial in South Africa
The National Institutes of Health and partners announce they will launch a large HIV vaccine trial in South Africa in November 2016, pending regulatory approval. This represents the first time since 2009 that the scientific community has embarked on an HIV vaccine clinical trial of this size.
January 14, 2017
Gates Foundation Invests in HIV-Prevention Implants
The Bill and Melinda Gates Foundation announces the investment of $140 million in a new HIV-prevention tool, implants that can deliver HIV-prevention medication continuously over a long period of time.
Learn More.
Eliminating the need for people to take preexposure prophylaxis (PrEP) medication on a daily basis, the HIV-preventing drug implants could be used to deliver a consistent supply of drugs, aiding people vulnerable to HIV.
“There’s a vital need for an HIV/AIDS intervention that allows those at risk to incorporate prevention more easily into their daily lives,” said Sue Desmond-Hellmann, CEO of the Bill & Melinda Gates Foundation.
May 2, 2017
CDC Reports Significant Decline in Death Rates in African Americans
The U.S. Centers for Disease Control and Prevention (CDC) reports significant declines in HIV/AIDS death rates for black/African Americans between 1999-2015. Among those aged 18-34, HIV-related deaths drop 80%, and among those aged 35, deaths drop by 79%.
June 6, 2017
America’s Black MSM Show Higher HIV Prevalence of Any Nation
The New York Times reports that, as a group, America’s black gay and bisexual men have a higher HIV prevalence rate than any nation in the world.
January 24, 2018
NIH Launches Study of Antiretrovirals & Pregnant Women
The National Institutes of Health launches a large international study to compare the safety and efficacy of antiretroviral treatment regimens for pregnant women living with HIV and their infants.
Learn More.
It will provide data on the use of newer HIV medications during pregnancy, helping to ensure that women living with HIV and their infants receive the best available treatments.
May 3, 2018
New Study: ART Key to Healthy Brain
An international research team finds that early antiretroviral therapy is key to avoiding brain atrophy for people living with HIV.
Learn More.
Researchers from the Montreal Neurological Institute and Hospital (The Neuro) of McGill University, in collaboration with researchers from University of Washington St. Louis and Yale University, analysed magnetic resonance imaging data from 65 patients at the University of California San Francisco who had been infected less than one year before. Assessment of the MRI data found that the longer people living with HIV went without treatment, the greater the atrophy in several brain regions.
Once patients began antiretroviral therapy, the atrophy stopped and some brain volume was even restored. These results underscored the need for early detection of HIV and delivery of ART as soon as possible to avoid neurological damage.
June 11, 2018
Early Antiretroviral Therapy Linked to Cancer Prevention
In the first study to focus specifically on the effect of viral suppression on cancer risk, researchers find that early, sustained ART helps to prevent cancers in people living with HIV.
Learn More.
The research shows that early and sustained ART reduces the onset of AIDS-defining cancers and — to a lesser degree — other cancers in HIV-positive people.
But the long-term study, which followed nearly 150,000 veterans over the years of 1999-2015, also found that the cancer risk for HIV-positive patients with long-term viral suppression still was greater than the risk of cancer for HIV-negative patients.
July 18, 2018
Studies Show HIV-Positive People Suffer from Heart Disease at 2x Rate
A global analysis finds that people living with HIV are twice as likely as their HIV-negative counterparts to suffer from heart disease.
The greatest impact is in sub-Saharan Africa and Asia Pacific regions, with Swaziland, Botswana and Lesotho particularly affected.
Researchers say the findings will help to target treatments to people facing the greatest risk, helping to maximize resources in countries with limited healthcare funding.
August 1, 2018
Computer Simulation Predicts Transmission Patterns Across Populations
Researchers at Los Alamos National Laboratory demonstrate that computer simulations can accurately predict the transmission of HIV across populations.
The simulations could allow state health departments to track the spread of HIV and provide a powerful new tool to help prevent new HIV infections.
“We looked for special genetic patterns that we had seen in the simulations, and we can confirm that these patterns also hold for real data covering the entire epidemic,” said Thomas Leitner, a computational biologist at Los Alamos and lead author of the study.
HIV is particularly interesting to study in this manner, Leitner noted, as the virus mutates rapidly and constantly within each infected individual. The changing “genetic signatures” of its code provide a path that researchers can follow in determining the origin and time frame of an infection, and the computer simulations are now proven to be successful in tracking and predicting the virus’s movements through populations.
September 28, 2018
Thai Study Confirms Accuracy of U=U Message
A study of MSM in Thailand finds that having a sexually transmitted infection does not affect the ability of people living with HIV to achieve and maintain an undetectable viral load, confirming that “Undetectable = Untransmittable.”
Learn More.
Months earlier, UNAIDS launched its “Undetectable = Untransmittable” (or U=U) campaign to spread the message that people living with HIV with an undetectable viral load cannot transmit HIV sexually.
UNAIDS’s campaign is supported by the results of three large studies of sexual HIV transmission among thousands of couples, one partner of which was living with HIV and the other was not, were undertaken between 2007 and 2016. In those studies, there was not a single case of sexual transmission of HIV from a virally suppressed person living with HIV to their HIV-negative partner.
October 17, 2018
Australian Study Links Diagnosis Reduction to PrEP
A research study finds that a targeted, high-coverage roll-out of PrEP (pre-exposure prophylaxis) is associated with a 25% reduction in new HIV diagnoses in one year.
The report concludes that rapid, targeted, high-coverage PrEP implementation is effective to reduce new HIV infections at the population level.
Less than a year later, Andrew Grulich, MD, head of the HIV Epidemiology and Prevention Program at the Kirby Institute at UNSW Sydney, would present follow-up data supporting the initial study at the 10th International AIDS Society Conference on HIV Science in Mexico City.
.
2019
NIH Develops Tool to Measure HIV Cure Strategies
Scientists funded by the National Institutes of Health (NIH) develop a tool to measure the success of HIV cure strategies.
Learn More.
The tool accurately and easily counts the cells that make up the HIV reservoir, the stubborn obstacle to an HIV cure. This advance has enabled researchers who are trying to eliminate the HIV reservoir to clearly understand whether their strategies are working.
The HIV reservoir consists of infected cells containing DNA molecules that encode HIV proteins, according to the NIH. In the reservoir, the HIV DNA (“provirus”) are in a resting state in which they are unable to generate new virus particles.
A team led by Robert F. Siliciano, M.D., at Johns Hopkins University School of Medicine analyzed DNA sequences from more than 400 HIV proviruses taken from 28 people with HIV. The scientists were able to categorize the HIV proviruses by two types of flaws: deletions and lethal mutations.
The researchers then developed strategically placed genetic probes that could distinguish the deleted or highly mutated proviruses from the intact ones. Finally, the scientists developed a nanotechnology-based method to analyze one HIV provirus at a time with these probes to determine how many proviruses in a sample are intact.
The researchers demonstrated that their method can readily and accurately measure the number of rare, intact proviruses that make up the HIV reservoir. The hope is that this new method will speed HIV research by allowing scientists to easily quantify the number of proviruses in an individual that must be eliminated to achieve a cure.
PrEP & Vaginal Ring Considered for Girls in Southern Africa
In a response to rising rates of infection among adolescent girls and young women in sub-Saharan Africa, the National Institutes of Health announces the launch of a clinical trial with girls and young women aged 16–21 at five sites in Kenya, South Africa, Uganda and Zimbabwe
Learn More.
The research project seeks to examine the safety and use of two HIV prevention tools — PrEP and a vaginal ring — for young women and girls under the title “REACH” (Reversing the Epidemic in Africa with Choices in HIV prevention).
One in four new infections in sub-Saharan Africa were women and girls aged 15-24 – despite making up 10% of the population.
“Women in less-developed countries disproportionately bear the burden in terms of ill health when facing food insecurity or a shock or disaster like drought that impacts the ability to get food or harvest food,” said Kelly Austin, associate professor of sociology at Lehigh University.
Essentially, lack of resources can lead to sexual assault, marriages of economic necessity and the resultant transmission of HIV.
Conducted for 1.5 years, the study would go on to show that the vast majority (97%) of the 247 participants used the vaginal ring and daily oral PrEP some or all of the time. Fewer than 3% of participants would use neither of the products, according to laboratory tests for adherence.
“In many ways, these results exceeded even our own expectations, yet at the same time, it’s not surprising to find that these young women have the capacity and desire to protect themselves against HIV,” explains Gonasagrie (Lulu) Nair, MBChB, MPH, REACH protocol chair, Centre for Medical Ethics and Law, Faculty of Medicine, at Stellenbosch University in South Africa. “They simply need to feel empowered and have the agency to make choices based on what they feel is right for them.”
March 4, 2019
‘London Patient’ Reportedly Second to be Cured of HIV
At the 2019 Conference on Retroviruses and Opportunistic Infections in Seattle, researchers announce the second cure of a person with HIV.
Learn More.
According to the case report published in Nature, an HIV patient in London has successfully received stem cell transplants of CCR5-delta 32, a rare genetic mutation that appears to make a small number of people resistant to HIV by preventing the virus from attacking the immune system.
The patient was diagnosed with non-Hodgkin’s lymphoma in 2012, which led his doctors to suggest gene therapy to create healthy blood cells. Since receiving the treatment, he has stopped taking antiretroviral medications and his body has reportedly been free of the virus for the past 18 months.
The patient, who is not named, is the second person to have successfully received such treatment. The first was Timothy Brown, a.k.a. the “Berlin Patient,” who made headlines in 2008 when he received a similar bone marrow transplant.
March 25, 2019
HIV-to-HIV Kidney Transplant Performed Successfully
Surgeons at Johns Hopkins Medical Center, perform the first living donor HIV-to-HIV kidney transplant in the U.S. The ability to use organs from living HIV-positive individuals could increase the supply available for transplant.
Learn More.
Nina Martinez, 35, is the living donor. She donated her kidney to an anonymous recipient after the friend she had hoped to give it to died last fall. Martinez acquired HIV when she was 6 weeks old through a blood transfusion and was diagnosed at age 8.
“I wanted to show that people living with HIV were just as healthy.” Martinez says in a news conference held to announce the medical break-through. “Someone needed that kidney, even if it was a kidney with HIV. I very simply wanted to show that I was just like anybody else.”
Martinez first learned of the opportunity for her to donate a kidney in 2013, when the HIV Organ Policy Equity Act (HOPE Act) passed in Congress. Yet, until she saw a storyline on the medical drama Grey’s Anatomy a few months later, she didn’t realize where her own life would intersect with kidney donation.
The HOPE Act was introduced on February 14, 2013, in the Senate by Sens. Barbara Boxer (D-CA), Tammy Baldwin (D-WI), Tom Coburn (R-OK), and Rand Paul (R-KY) and in the House by Rep. Lois Capps (D-CA). The Senate passed the legislation by unanimous consent, and about six months later, the House passed it by unanimous consent.
“This is the first time someone living with HIV has been allowed to donate a kidney, ever, in the nation, and that’s huge,” says Dorry Segev, M.D., Ph.D., professor of surgery at Johns Hopkins. “A disease that was a death sentence in the 1980s has become one so well-controlled that those living with HIV can now save lives with kidney donation — that’s incredible.”
May 19, 2019
NIH Evaluates Antiretroviral Therapy for HIV Suppression
A clinical trial is launched to evaluate long-acting ART (antiretroviral therapy) for maintaining HIV suppression in people who find it a challenge to take a daily medication.
Learn More.
The National Institutes of Health study, called Long-Acting Therapy to Improve Treatment Success in Daily Life (LATITUDE), will help determine whether a combination of two experimental injectable formulations of ART are better than conventional daily medications in managing HIV infection in certain populations.
The purpose of this study, supported by funding is to compare the efficacy, safety, and durability of two different strategies to treat participants with a history of sub-optimal adherence and control of their HIV infection: long-acting antiretroviral therapy (ART) and all-oral standard of care (SOC).
LATITUDE seeks to enroll approximately 350 volunteers with documented treatment lapses within the past 18 months. All study participants will begin a daily oral ART regimen and individualized adherence and retention support. Volunteers who become virally suppressed by week 24 will then be randomized to either continue standard-of-care therapy for one year or begin an oral regimen consisting of RPV and CAB for 4 weeks, followed by long-acting injectable formulations of those drugs every 4 weeks for 48 weeks.
After this 52-week period, participants originally randomized to the standard-of-care arm may cross over to long-acting therapy, and participants originally randomized to the long-acting therapy arm may remain on that regimen for an additional year.
Report: HIV-related Deaths in U.S. Shrink between 2007 and 2018
While HIV remains among the 10 leading causes of death among certain populations, deaths among persons with diagnosed HIV (PWDH) decreased 48% between 2010 and 2017, according to a report issued by the Centers for Disease Control and Prevention (CDC).
Learn More.
The CDC published in the Morbidity and Mortality Weekly Report a new study showing that the rate of HIV-related deaths among people with HIV in the U.S. fell by nearly half from 2010 to 2017. The reduction was attributed to the increase in early testing and diagnoses of people with HIV and helping them to get – and stay on – lifesaving treatment.
With retroviral treatment available to extend the lives of PWDH, HIV nonetheless remained a top cause of death in certain U.S. populations. The rate of HIV-related deaths was highest in the South (6.0 per 1,000 PWDH) and lowest in the Northeast (3.2 per 1,000 PWDH).
Rates of HIV-related deaths during 2017 were higher among females (5.4 per 1,000 PWDH) than males (4.5) and transgender females (4.3), and highest among persons of multiple races (7.0) and Black persons (5.6), followed by White persons (3.9) and Hispanic/Latino persons (3.9)
During 2017, rates of HIV-related deaths by race/ethnicity varied by jurisdiction. Rates of HIV-related death were highest among White persons in South Carolina (10.1), Oklahoma (7.5), and Arkansas (6.5); highest among Black persons in Mississippi (11.5), Louisiana (8.8), South Carolina (8.2), and Nevada (8.2); and highest among Hispanic/Latino persons in Puerto Rico (9.2), Texas (6.5), and Arizona (6.2).
_ _ _ _ _ _
Source: Bosh KA, Johnson AS, Hernandez AL, et al. “Vital Signs: Deaths Among Persons with Diagnosed HIV Infection, United States, 2010–2018,” Morbidity and Mortality Weekly Report (MMWR), November 20, 2020.
December 7, 2020
Viral Suppression Success Rate Hits New High for Clients of Ryan White Program
Clients receiving medical care through the Ryan White HIV/AIDS Program were virally suppressed at a record level – 88.1% – in 2019, according to a report released by the U.S. Health Resources & Services Administration (HRSA).
Learn More.
The Health Resources & Services Administration (HRSA) attributed the significant increase in viral suppression to the Ryan White HIV/AIDS Program’s effectiveness in providing timely HIV diagnosis, care, and treatment of HIV to the country’s most vulnerable populations.
The program serves People Diagnosed with HIV (PDWH) who are low income and have insufficient health insurance to cover needed treatment and care. Almost one-third of the clients in 2019 were aged 55 years and older. As the largest federal program focused exclusively on HIV services for more than a half a million people, the Ryan White program was funded at $2.32 billion in fiscal year 2019.
In 2019, about 88% of 370,119 patients had a suppressed viral load at their most recent test, according to the HRSA’s 2019 Ryan White HIV/AIDS Program (RWHAP) Client-Level Data Report. From 2015 through 2019, the number of patients receiving AIDS/HIV services who also received a viral load test increased by more than 30,000. Despite significant increases in OAHS patients, the overall percentage of patients with viral suppression also increased, from 83.4% in 2015 to 88.1% in 2019.
The age group making the greatest progress in viral suppression from 2015 to 2019 was young people aged 15-24. However, lower rates of viral suppression among transgender youth (73.8%) and youth with unstable housing (69.3%) indicated that these populations require more outreach and attention, according to the report.
“Although anyone can have HIV, all people and communities are not impacted equally,” the report stated. “The HRSA HIV/AIDS Bureau has enhanced its efforts to focus on populations where HIV is most concentrated. These key populations include women; transgender women; gay, bisexual, and other MSM; Blacks/African Americans; Hispanics/Latinos; youth; young, Black/African American MSM; young, Black/African American women; and people with HIV infection attributed to injection drug use, and people with unstable or temporary housing.”
First Injectable, Extended Release HIV Treatment is Approved for Distribution
The Food and Drug Administration approves Cabenuva, the first alternative to a daily oral HIV treatment regimen.
Learn More.
The FDA’s approval of Cabenuva (cabotegravir and rilpivirine, in an injectable formulation) made it the first time an injectable, extended release, complete HIV treatment regimen was available in the U.S.
For many HIV-infected adults who were virologically suppressed on a stable antiretroviral regimen, Cabenuva replaced their daily oral antiretroviral regimen with a once-a-month injection.
“This approval will allow some patients the option of receiving once-monthly injections in lieu of a daily oral treatment regimen,” said John Farley, M.D., M.P.H., director of the Office of Infectious Diseases in the FDA’s Center for Drug Evaluation and Research. “Having this treatment available for some patients provides an alternative for managing this chronic condition.”
The FDA also approved Vocabria (cabotegravir, tablet formulation), which is taken in combination with oral rilpivirine (Edurant) for one month prior to starting treatment with Cabenuva to ensure the medications are well-tolerated before switching to the extended-release injectable formulation.
The safety and efficacy of Cabenuva were established through two randomized, open-label, controlled clinical trials in 1,182 HIV-infected adults who were virologically suppressed (HIV-1 RNA less than 50 copies/milliliter) before initiation of treatment with Cabenuva, according to the FDA. Patients in both trials continued to show virologic suppression at the conclusion of each study. Cabenuva and Vocabria were granted Fast Track and Priority Review designation by the FDA.
In March 2022, the FDA would approve the use of Cabenuva for adolescents, extending the treatment option to HIV-infected people as young 12 years old, as long as they weigh at least 77 pounds and are already on a stable antiretroviral regimen, with no history of treatment failure, nor known or suspected resistance to either cabotegravir or rilpivirine
January 21, 2021
FDA Approves Cabenuva, First Injectable Extended-Release HIV Regimen
The Food & Drug Administration approves Cabenuva, the first injectable, extended-release, complete HIV treatment regimen.
Learn More.
Designed to replace a daily regimen of antiretroviral therapy, Cabenuva was the first FDA-approved ounce-a-month injectable regimen for HIV-infected adults.
“With the approval of Cabenuva, we’re proud to bring a new treatment option to people living with HIV that removes the burden of taking a daily pill,” said Paul Stoffels, M.D., Vice Chairman of the Executive Committee and Chief Scientific Officer at Johnson & Johnson. “While much more remains to be done to make HIV history, today’s milestone reminds us how far medical innovation has come since the first reported cases of the virus almost 40 years ago.”
The FDA also approved Vocabria, which was developed to be taken in combination with oral rilpivirine for one month prior to starting treatment with Cabenuva to ensure the medications are well-tolerated before switching to the extended-release injectable formulation.
Cabenuva and Vocabria were granted Fast Track and Priority Review designation by the FDA. Fast track is a process designed to expedite the review of drugs to treat serious conditions and fill an unmet medical need. This process can be traced back to the early 1990s, when advocates for the HIV/AIDS community demanded that researchers and government agencies work harder to get important new drugs — some of them still considered experimental — to patients faster. Back then, it could take an average of 12 years for a drug to progress from the research lab to FDA approval.
“Currently, the standard of care for patients with HIV includes patients taking daily pills to adequately manage their condition. This approval will allow some patients the option of receiving once-monthly injections in lieu of a daily oral treatment regimen,” said John Farley, M.D., M.P.H., director of the Office of Infectious Diseases in the FDA’s Center for Drug Evaluation and Research. “Having this treatment available for some patients provides an alternative for managing this chronic condition.”
The FDA approval followed the success of two randomized, open-label, controlled clinical trials in 1,182 HIV-infected adults who were virologically suppressed before starting treatment with Cabenuva. Patients in both trials continued to show virologic suppression at the conclusion of each study, and no clinically relevant change from baseline in CD4+ cell counts was observed.
_ _ _ _ _
Sources: U.S. Food and Drug Administration, press release dated January 22, 2021
Janssen Pharmaceutical Companies of Johnson & Johnson, press release dated January 21, 2021
March 10, 2021
CDC Study Reveals Racial/Ethnic Disparities in COVID Response
Similar to the HIV/AIDS epidemic in the U.S., the COVID-19 pandemic continues to deepen health disparities among racial and ethnic lines across the country, according to a report by the Centers for Disease Control and Prevention.
Learn More.
Using multiple sources, CDC data illustrated how the risks for COVID-19 illness, hospitalization, and death differ by race and ethnicity.
Indigenous Americans (native American and Alaska native people) were almost four times more likely than non-Hispanic white people to be hospitalized and more than twice as likely to die from COVID-19 infection.
Black people were almost three times more likely than non-Hispanic white people to be hospitalized and almost twice as likely to die from COVID-19 infection.
Hispanic and Latino people were more than three times more likely than non-Hispanic white people to be hospitalized and more than twice as likely to die from COVID-19 infection.
In this study of young people, the largest persistent disparities involved Indigenous Hawaiian and Pacific Islander, Indigenous American, and Hispanic persons.
As of this date, 95.7 million vaccine doses had been administered, according to the CDC.
June 5, 2021
CDC’s Initial Report of AIDS Turns 40
The world marks 40 years since the first five cases of what later became known as AIDS were officially reported in Los Angeles.
On this day, the Foundation for The AIDS Monument held its ceremonial groundbreaking at the future site of STORIES: The AIDS Monument in West Hollywood Park. Among the community members who attend the event is Dr. Michael Gottlieb, one of the authors of the June 1981 CDC report announcing the first five cases of an illness subsequently defined as acquired immunodeficiency syndrome (AIDS).
The five men described in the report were between the ages of 29-36 and resided in the Los Angeles area, and by the time the report was published, two had already died. The relatively brief report gave scant information about this new medical phenomenon, including the following:
The patients did not know each other and had no known common contacts or knowledge of sexual partners who had had similar illnesses.
Two of the five reported having frequent homosexual contacts with various partners.
All five reported using inhalant drugs, and one reported parenteral drug use (i.e., injected or implanted drugs).
June 7, 2021
Person Diagnosed with HIV Becomes U.S. AIDS Czar
The White House announces the appointment of Harold J. Phillips, an out gay man living with HIV since 2005, to lead the Office of National AIDS Policy (ONAP).
[Photo courtesy of the U.S. Department of Health & Human Services]
Learn More.
Ambassador Susan Rice, White House Domestic Policy Advisor and head of the Domestic Policy Council, made the announcement in a Twitter thread recognizing the 40th anniversary of the publication of the first reports of what later became known as AIDS. ONAP is part of the Domestic Policy Council.
“I’m thrilled to welcome Harold Phillips to lead the White House Office of National AIDS Policy. Harold brings decades of experience in the battle against HIV/AIDS, and we’re lucky to have him spearheading the Biden-Harris Administration’s efforts to defeat this epidemic … I know Harold and ONAP will be instrumental to that effort,” Rice wrote in her Tweet.
Phillips was a longtime public health official whose most recent position was the Senior HIV Advisor and Chief Operating Officer of the Ending the HIV Epidemic (EHE) initiative in the Office of Infectious Disease and HIV/AIDS Policy at the U.S. Department of Health and Human Services.
Prior to his HHS position, Phillips served as the Director of the Office of HIV/AIDS Training and Capacity Development at the Health Resources and Service Administration’s HIV/AIDS Bureau, where he had previously served as Deputy Director of the Ryan White HIV/AIDS Program and AIDS Drug Assistance Programs.
In addition, he previously worked at NMAC and served on the CDC/HRSA Advisory Committee on HIV, Viral Hepatitis and STD Prevention and Treatment from 2003–2010.
On his first day as Director of ONAP, Phillips told his colleagues, “I look forward to continuing the work we have begun to end the HIV epidemic. President Biden is committed to ending the HIV epidemic and has called for bold and accelerated steps to achieve this aim.”
He shared that as part of those efforts, ONAP would lead the development of a new National Strategy on HIV/AIDS which updates the HIV National Strategic Plan released in January 2021. This new strategy would be released less than six months later and build on the previous administration’s plan.
“As a uniquely and unapologetically Black organization that has led the fight to end HIV for 22 years, Harold is just as much a part of our community as he is the highest-ranking Black HIV leader in the federal government,” said Raniyah Copeland, President and CEO of the Black AIDS Institute, in response to the announcement.
“I am hopeful that Harold’s leadership and the Biden-Harris administration’s recognition of racism as a public health issue will be a catalyst to finally center Black lives,” Raniyah said.
ONAP had not had leadership since President Donald Trump took office in 2017. Following the inauguration of Trump, the ONAP website became inaccessible and it was reported the office was closed with the departure of the previous director, Amy Lansky. The office continued to lie dormant for several months, during which time six members of the Presidential Advisory Council on HIV/AIDS (PACHA) filed letters of resignation.
One of the resigning council members, Scott A. Schoettes of Lambda Legal, toldNewsweek: “The Trump Administration has no strategy to address the on-going HIV/AIDS epidemic, seeks zero input from experts to formulate HIV policy, and — most concerning — pushes legislation that will harm people living with HIV and halt or reverse important gains made in the fight against this disease.”
The five other members of PACHA who resigned on June 13, 2017 were Lucy Bradley-Springer, Gina Brown, Ulysses W. Burley III, Michelle Ogle, and Grissel Granados, citing that the Trump administration “simply does not care” about the HIV/AIDS situation in the U.S.
In December 2017, Trump fired all the remaining members of the council, and it was more than a year before he would name nine new members to the council.
August 23, 2021
FDA Fully Approves Pfizer COVID-19 Vaccine
The Food and Drug Administration fully approves the Pfizer-BioNTech COVID-19 vaccine for people aged 16 and older, following a manufacturing review and analysis of the company’s expanded clinical trial.
Learn More.
Up until this day, the vaccines available in the U.S. — made by Pfizer and BioNTech, Moderna, and Johnson & Johnson — have been authorized on “an emergency basis” but had yet to be fully approved.
A fully approved COVID vaccine was particularly important to members of the HIV community, because people with HIV have higher rates of certain underlying health conditions, particularly if they are aged 50 or older.
The Pfizer-BioNTech vaccine, which was marketed as Comirnaty, was the first COVID-19 vaccination to receive full review and approval from the U.S. regulatory agency. The FDA would approve the vaccine’s use in children aged 5-11 the following October.
The company’s clinical trial included approximately 44,000 participants and found the vaccine to be 91% effective in preventing COVID-19 disease.
“National Institute of Allergy and Infectious Diseases (NIAID) inventors and their collaborators had already developed a stabilized prefusion coronavirus spike protein that could be used as a vaccine antigen to cause neutralizing antibody responses,” stated the NIH in its feature on Comirnaty. “NIH’s ongoing research allowed for BioNTech/Pfizer to quickly develop a vaccine and bring it to market based on NIH technologies.”
Previously, in December 2020, the Pfizer-BioNTech vaccine was granted emergency use authorization by the FDA in response to the public health emergency posed by the coronavirus pandemic. That authorization involved a review of safety data on over 37,000 participants in a randomized, placebo-controlled study.
“While millions of people have already safely received COVID-19 vaccines, we recognize that for some, the FDA approval of a vaccine may now instill additional confidence to get vaccinated,” said Dr. Janet Woodcock, the then acting FDA Commissioner. “Today’s milestone puts us one step closer to altering the course of this pandemic in the U.S.”
The FDA’s approval came amidst the spread of the highly contagious COVID-19 delta variant across the country. It also represented a turning point in U.S.’s response to COVID-19, as more private and public entities began instating vaccination requirements to stem the spread of COVID-19.
“The new vaccine was the result of months of work, robust data evaluation and a thorough, comprehensive review process that has protected more than 100 million Americans from severe COVID-19 complications,” said the American Medical Association in its newsletter. “It is a milestone and major step forward in the worldwide effort to end this pandemic.”
Among those who adopted vaccine mandates for employees in the wake of the Pfizer-BioNTech vaccine’s FDA approval were the Pentagon and the New York City school system.
December 21, 2021
FDA Approves First Long-Acting Injectable form of PrEP
The Food and Drug Administration approves Apretude, the first long-acting injectable form of HIV pre-exposure prophylaxis (PrEP) for use in adults and adolescents.
Learn More.
The FDA approval of the distribution of Apretude (cabotegravir extended-release injectable suspension) expands the HIV prevention options available to people in the U.S. The one-every-two-month injection is a viable and, for many, more convenient alternative to daily oral pills.
In a trial with 4,566 men and transgender women who have sex with men, participants received Apretude or Truvada (a daily PrEP medication). According to the FDA, the trial results showed that those who took Apretude had a 69% less risk of getting infected with HIV, compared to those who took Truvada.
A second trial was held with 3,224 cisgender women who received either Apretude or Truvada, and those who took Apretude had a 90% less risk of getting infected with HIV versus those who took Truvada.
“This injection, given every two months, will be critical to addressing the HIV epidemic in the U.S., including helping high-risk individuals and certain groups where adherence to daily medication has been a major challenge or not a realistic option,” Debra Birnkrant, director of the Division of Antivirals in the FDA’s Center for Drug Evaluation and Research, told USA Today.
Injectable cabotegravir PrEP, which is administered by a healthcare worker every two months, is indicated for adults and adolescents weighing at least 77 pounds to reduce the risk of sexually acquired HIV. It is approved for cisgender and transgender men and women with no limitations based on the type of sex they have, according to the FDA as reported in AIDSMap.
While this news sounds great for those who seeking an injectable PrEP option, paying for Apretude could be daunting for those whose health insurance doesn’t cover the cost of the medication.
While the federal government mandated in July 2021 that health insurers must cover the cost of the PrEP pills Truvada and Descovy (as well as the lab tests and clinic visits required to maintain these prescriptions), insurance companies were at that time not required to cover all the costs for Apretude — which had a list price of $3,700 per dose, plus additional clinic fees for administering the injection, according to NBC News.
February 3, 2022
Highly Virulent HIV-1 Variant Discovered in Netherlands
Found in 109 people in the Netherlands, a new HIV variant is determined to be more than five times more virulent than previous forms of HIV, making those infected that much more infectious.
Learn More.
People infected with this variant were also found to undergo a twice-as-fast deterioration of their immune system, setting them on a course to potentially develop AIDS years earlier than people with other versions of HIV, according to a report in Science magazine released on this day.
HIV-1 virulence is most commonly measured by viral loads (the concentration of viral particles in blood plasma) and CD4 counts (the concentration of T cells). Successful treatment of HIV-1 with antiretroviral drugs is indicated by the suppression of the viral load and interruption of the decline in CD4 counts that would otherwise lead to AIDS.
The study of the 109 individuals in the Netherlands with subtype-B HIV-1 found that the new variant carries more than 500 mutations scattered across its genome — though it was unclear how the mutations were able to manifest as a more severe form of the disease.
The study also finds that this variant still responds to current HIV treatments.
“Our discovery of a highly virulent and transmissible viral variant … emphasizes the importance of access to frequent testing for at-risk individuals and of adherence to recommendations for immediate treatment initiation for every person living with HIV,” wrote the lead researcher for the study, Chris Wymant, the senior researcher in statistical genetics and pathogen dynamics at the Oxford Big Data Institute.
Individuals with the variant were mostly men who have sex with men (82%), similar to non-variant HIV-positive individuals (76%). Age at diagnosis was also similar for variant and non-variant individuals; neither ethnicity nor host genotype data were available, but the place of birth was mostly recorded as Western Europe for both groups (71% for non-variant individuals, 86% for variant individuals).
A genetic sequence analysis conducted by the researchers indicated that the variant emerged some time in the 1990s from de novo mutation (an alteration as a result of a mutation on the cellular level), not recombination (the process by which chromosomes exchange genetic material).
While the variant spread quickly during the 2000s, its infection rate has been declining since around 2010 — probably as a result of the country’s access to life-saving treatment and efforts to curb HIV transmission, Wymant told Nature magazine.
Falsehoods on Social Media Claim HIV-COVID Vaccine Connection
False rumors spread online claim the newly discovered, highly virulent variant of HIV circulating in the Netherlands was “created” by COVID-19 vaccines.
Learn More.
One Twitter user wrote: “What will you do when it is found that HIV is in the vaccine via Spike protein? New HIV strain found in the Netherlands: Highly infectious variant makes people ill twice as quick. There are no coincidences!”
“A serious outbreak of HIV cases found in the Netherlands. Source – Daily Mail. Any connection with the Covid jabs, I wonder? This has Fauci written all over it,” reads another tweet.
“While recently identified, the ‘VB variant’ predates de COVID-19 pandemic and patients analyzed in the paper were infected between the 2000s and early 2010,” Reuters reported.
Reuters had previously addressed other allegations around false narratives that COVID-19 vaccines caused HIV or that the SARS-CoV-2 virus was developed with a genetic code of HIV. The most recent HIV-COVID falsehoods are related to a research study published on Feb. 3, 2022 in the journal Science, which identified a “highly virulent variant of subtype-B HIV-1.”
“There is absolutely no basis to the claim of an association between COVID, or COVID vaccination, and the severity of infection in those infected with the VB variant of HIV,” senior author Professor Christophe Fraser from the University of Oxford’s Big Data Institute and Nuffield Department of Medicine, told Reuters via email.
“Such an association is strictly impossible due to the timing of when the data were collected and analyses, and when the patients were infected,” he said.
The study stated that genetic sequence analysis suggests the variant manifested some time in the 1990s.
Fraser told Reuters how he and the other researchers were able to trace the variant back 30 years: “Using the genetic diversity of the viruses within the lineage, we constructed a family tree of the viruses, and used a molecular clock to date the emergence.”
Furthermore, most of the cases analyzed in the study were diagnosed in the 2000s and early 2010s, he added.
February 8, 2022
Luc Montagnier, Scientist Who Discovered Cause of AIDS, Dies at 89
Luc Montagnier, the French scientist who won a Nobel prize with his colleague Françoise Barré-Sinoussi for discovering HIV, dies at the age of 89.
Learn More.
Montagnier’s work on HIV made it possible for scientists to develop diagnostic tests and treatments that have saved countless lives.
Montagnier worked in several laboratories before landing at the Pasteur Institute in Paris in 1972, according to Heidi Ledford’s article in Nature magazine. After developing an expertise in virology, he began to specialize in retroviruses, which are viruses with an enzyme capable of making a complementary DNA copy of the viral RNA, and then integrating it into the host cell’s DNA.
This knowledge made Montagnier the right researcher in the right place in January 1983, when a colleague sent him lymph node tissue taken from a French fashion designer thought to be in the early stages of AIDS.
When other scientists began releasing studies showing the depletion of a class of immune cells (CD4+ T cells) in people with AIDS, Montagnier took note. He knew of a retrovirus that infected CD4+ T cells, and it was transmitted through blood and sexual activity. He had a hunch that AIDS was caused by a retrovirus, too.
Working on Montagnier’s instincts, Françoise Barré-Sinoussi was able to isolate a new retrovirus from the lymph node biopsy. It was a major breakthrough for Montagnier’s virology unit at the Pasteur Institute — they had found the cause of AIDS.
Montagnier’s team — which called the viral isolates LAV, for Lymphadenopathy Associated Virus — published its research results in Science magazine on May 20, 1983. Four months later, Montagnier presented the results to a skeptical audience at a small, late-night session of a scientific conference at Cold Spring Harbor Laboratory in New York organized by Robert C. Gallo, M.D. a top researcher at the National Institutes of Health’s National Cancer Institute.
“Mentally, most attendants were not prepared to accept the idea of a second family of retroviruses … existing in humans and causing immune deficiency, and having no counterpart in animals!” Montagnier wrote in 2008 in his Nobel prize biography. “This situation is not infrequent in science, since new discoveries often raise controversy.”
About a year after the Cold Spring Harbor conference, Dr. Gallo announced that he had discovered the cause of AIDS in the family of T-cell lymphotropic viruses (HTLVs), in a virus he called HTLV-III. Later, this virus was found to be virtually identical to the Pasteur Institute’s LAV, according to the Mayo Clinic’s biography of Montagnier.
The separate claims of discovery by Montagnier and Gallo culminated in a lawsuit in December 1985. Virology icon Dr Jonas E. Salk stepped in to mediate the conflict and the two researchers finally resolved their differences.
in 1986, the AIDS virus was officially designated as human immunodeficiency virus (HIV). Both researchers were recognized and honored by the Lasker Foundation and received the 1986 Albert Lasker Medical Research Award. The Foundation cited Montagnier for “discovery of the [AIDS] retrovirus later shown to be responsible for the major new threat to world health,” and Gallo was acknowledged as the originator of much human retrovirus research.
In March 1986, Montagnier and his team announced the discovery of HIV-II, another strain of the AIDS virus. They reported further isolates from AIDS patients, including a heterosexual couple from Africa and later from hemophiliacs, according to Robin A. Weiss and Simon Wain-Hobson in Science magazine.
Using tissue samples from key clinical researchers, Montagnier’s team was successful in developing lab tests for HIV antibodies, which enabled the development of blood tests to diagnose HIV infection.
Montagnier received many awards, including a Chevalier de la Légion d’ Honneur in 1984 and the Commandeur de l’Order National du Mérite in 1986 as well as professional honors from Switzerland, Canada, and Japan. He was honored on a stamp issued by Bhutan in 2000.
According to Nature, Montagnier spent his later years dismantling his hard-won reputation as a top scientist by opposing vaccination during the COVID-19 pandemic.
February 22, 2022
New HIV Variant Heightens Concerns about COVID’s Progression
A more virulent and transmissible HIV variant discovered in the Netherlands causes concern that SARS-CoV-2, the coronavirus that causes COVID-19, could likewise evolve very quickly into more potent variants.
Learn More.
With the world of science fixed on the COVID pandemic, it is easy to overlook the AIDS-related death toll at an estimated 650,000 worldwide in 2021. But the endurance of HIV is remarkable and may have something to reveal about the future of COVID.
With 43.8 million people worldwide living with HIV in 2021 (of them, an estimated 2 million infected in the last year), one researcher is studying a strain of HIV that might predict the path that the corona virus may take in the months and years to come, according to Scientific American.
William A. Haseltine, an infectious disease researcher who founded Harvard University’s cancer and HIV/AIDS research departments and now chairs the think tank ACCESS Health International, told Scientific American about his theories about corona virus mutations and linked it to the recently identified virulent HIV variant.
The new HIV variant is thought to have a potency of more than five times previous variants, making those infected with the variant that much more infectious. Plus, people infected with this variant often suffer a twice-as-fast deterioration of their immune system, setting them on a course to potentially develop AIDS years earlier than people with other versions of HIV.
These findings, published earlier in the month in Science magazine, indicate that the new variant carries more than 500 mutations scattered across its genome — though it is unclear how they enable the virus to cause more-severe disease.
“We’ve known that all viruses adapt. The way they adapt is much like how we use artificial intelligence to solve complex problems: the machine throws a lot of random combinations at something, and the one that works best is the one that survives,” Haseltine explained.
The evolution of HIV has been “a long, drawn-out process,” because the virus is poorly transmissible and in some cases can take a year or more to spread from one person to another, he said. However, the corona virus can be transmitted quite quickly and easily — “by a person simply breathing the air somebody else breathed a half an hour ago” — and that quick transmission process is conducive to the virus evolving into different forms.
“What the virus wants to do is get from one person to another—get in and get out,” Dr. Haseltine told Scientific American. “Because HIV is so poorly transmitted, its best strategy is to get in and stay there for a very long time and rely on a predictable behavior — sex — to get out.”
By comparison, the corona virus survives by reinfecting people who have been infected in the past, he said.
“There are many ways for this virus to mutate to increase its transmissibility,” said Haseltine. “Whether any of those will affect virulence is unclear.”
Haseltine has written extensively about the potential of SARS-CoV-2 to evolve into a much more dangerous strain.
June 16, 2022
HHS Awards $115M to HIV Care Programs in Target Areas
The U.S. Department of Health and Human Services (HHS) awards nearly $115 million to 60 recipients with innovative strategies to help people with HIV access care, support, and treatment services. Los Angeles County received one of the largest awards.
The county’s EHE initiative was aligned with the federal EHE initiative, which sought to reduce the number of new HIV infections in the U.S. by at least 90% by 2030. At the time, new HIV cases in LA County represented more than 5% of the total number of cases in the country.
“With this investment, we’re increasing our efforts to end the HIV epidemic,” said HHS Secretary Xavier Becerra. “Today’s awards reaffirm our Ryan White HIV/AIDS Program work in communities that need it most as we continue to ensure everyone with HIV receives the care they need to thrive.”
The funding arrives through the federal Ryan White HIV/AIDS Program, which provides services to low-income people living with and at risk for HIV, according to an HHS press release. About 560,000 people with HIV in the U.S. receive services through the program.
“That’s nearly half of the 1.2 million people with the virus,” Trent Straube wrote in POZ magazine. “What’s more, 88% of people receiving care through the Ryan White program attain viral suppression. People with an undetectable viral load not only enjoy longer and healthier lives but also do not transmit HIV through sex.”
November 3, 2022
AIDSVu Releases 2020 Data on HIV
AIDSVu releases its annual report, including interactive maps and data visualizing the HIV epidemic at the state and county levels, showing that there were 30,632 new HIV diagnoses in the U.S. in 2020 (a likely undercount due to the impact of the COVID).
Learn More.
The updated maps from AIDSVu, alongside the organization’s new HIV care continuum maps stratified by race/ethnicity, show continued disparities in access to treatment and care across different geographies and communities.
AIDSVu is a project by Emory University’s Rollins School of Public Health to make HIV data widely available, easily accessible, and locally relevant to inform public health decision-making and action. Operating since 2010, Emory University coordinates this work in partnership with Gilead Sciences, Inc. and the Center for AIDS Research at Emory University.
This year’s maps serve as a snapshot of the HIV epidemic during the beginning of the COVID-19 pandemic, which impacted resources, HIV testing, HIV new diagnoses, and data collection over the last two years.
New to this year’s report were data from Funders Concerned About AIDS that tracks philanthropic HIV funding across the U.S. These data provide insights about the use of funds granted for advocacy, social services, prevention, and treatment in Ending the HIV Epidemic (EHE) Initiative focused jurisdictions and in specific communities most impacted by HIV.
The AIDSVu website provides researchers, policymakers, and community members with a more comprehensive understanding of the HIV epidemic at the local, state, and national level. The data displayed on AIDSVu were obtained from the CDC and compiled by researchers at the Rollins School of Public Health. Additional data (ZIP Code, census tract, and community area/ward data) were provided by state and city health departments and compiled by researchers at the Rollins School of Public Health.
“Looking at 2020 HIV data, it is impossible to avoid the fact that COVID-19’s impact has been wide-ranging,” said Patrick Sullivan, DVM, PhD, Professor of Epidemiology at Emory University’s Rollins School of Public Health and Principal Scientist for AIDSVu. “While we are still trying to understand the full extent of the impact COVID-19 had on testing, treatment, and care, this data will help enable that conversation,”
Dr. Sullivan also said that the maps illustrate that there is still much work to be done before the HIV epidemic can be eradicated.
February 1, 2023
Revised Guidelines Support Breastfeeding Rights
After years of studies that show mother-to-infant HIV transmission during breastfeeding is unlikely to occur when the mother has a sustained undetectable viral load, the U.S. updates its HIV clinical practice guidelines to clarify breastfeeding options.
Learn More.
The Office of AIDS Research from National Institutes of Health announced updates to the federal HIV clinical practice guidelines, which previously discouraged HIV-positive people from breastfeeding/chestfeeding infants.
The updated guidelines refrained from taking a stand on whether to breastfeed/chestfeed, and instead sought to quantify the risk of HIV transmission against the risk of formula, so that people with HIV could weigh the risks themselves with the help of a healthcare professional, according to the NIH.
The updated guidelines note that:
The risk of HIV transmission while breastfeeding is less than 1% (but not zero) for PWH on antiretroviral therapy (ART) with sustained undetectable viral load through pregnancy and postpartum.
The risk of postnatal HIV transmission to an infant is zero with the use of safe replacement feeding. Properly prepared formula or pasteurized human donor milk from a milk bank eliminates risk of HIV transmission to the infant.
Clinicians should support the choices of people with HIV to breastfeed (if they are virally suppressed) or to formula/replacement feed.
It is inappropriate to engage Child Protective Services or similar services in response to infant feeding choices of a person with HIV.
“If you are a woman living with HIV in an area of the world where access to resources like clean water, refrigeration, and medical care are limited, the World Health Organization (WHO) recommends that you breastfeed if you are taking HIV drugs,” The Well Project stated in its article “Can I Breastfeed While Living With HIV?”
“A course of HIV drugs may also be recommended for the baby during breastfeeding. The reason for this recommendation is that, in such resource-limited settings (for instance, many areas of Africa or India), infants are more likely to develop diarrhea and other illnesses, and may die from these,” the article continued.
“Breast milk contains substances that protect and strengthen a child’s immune system, even after they stop breastfeeding. Because of this, breast milk may help children to survive these health conditions. Furthermore, formula feeding may not be an option in these areas due to lack of funds to purchase it, clean water to mix it with (if the formula is powdered), or refrigeration to keep it fresh. Health authorities have determined that the benefits of breastfeeding outweigh the risks of HIV in areas where resources are constrained in this way.”
February 21, 2023
NIH Studies HIV Treatment for Those Most At-Risk
Promising results come from a study designed to provide a viable antiretroviral treatment plan for HIV-positive people living on society’s fringe.
Learn More.
The study, which was supported by the National Institutes for Health, found that that long-acting antiretroviral therapy (LA-ART) can benefit people who face many treatment barriers due to housing insecurity, mental illnesses, and substance use disorders
Injectable ART given every four to eight weeks, and delivered with comprehensive support services, was successful in suppressing HIV in almost all of the trial’s 133 participants, 57 of whom were previously not virologically suppressed, according to the NIH.
The results indicate that injectable ART can provide better health outcomes for people who are not able to manage treatment that requires daily pills.
The findings were presented at the Conference on Retroviruses and Opportunistic Infections by Monica Gandhi, M.D., professor of medicine and associate division chief at the University of California, San Francisco, and medical director of Ward 86 at San Francisco General Hospital.
“Our patient population does not look like the patient population that got enrolled in the clinical trials to determine the approval criteria for long-acting ART,” said Dr. Gandhi. “It is the role of researchers to help address disparities through intentionally and proactively including diverse groups in our studies, and for this population to have the same successful outcomes as those in the other clinical trials was very important and exciting.”
The results showed the following:
Among 76 participants who began the study with virologic suppression, all (100%) remained suppressed over the period of research follow-up phase.
Among the 57 participants who did not begin the study with virologic suppression, 55 (96.5%) had achieved virologic suppression.
Only two of the 133 study participants did not achieve or maintain viral suppression, a rate of 1.5%, in line with findings from previous clinical trials that studied LA-ART in people with HIV who had achieved viral suppression on daily oral ART.
Participants had a median age of 45, and 58% reported having unstable housing, 8% reported experiencing homelessness, 38% reported having a mental illness, and 33% reported substance use.
July 28, 2023
NIH: Statin Reduces Heart Disease Risk among HIV+ Adults
A daily statin may significantly offset the elevated risk of heart disease experienced by people living with HIV by more than a third, according to research released by the National Institutes of Health.
Learn More.
The NIH-supported study indicated that statins reduce the risk of heart disease in HIV+ people by more than a third, potentially preventing one in five major cardiovascular events or premature deaths in this population.
People living with HIV have a 50-100% increased risk for cardiovascular disease, according to the NIH.
“This research suggests that statins may provide an accessible, cost-effective measure to improve the cardiovascular health and quality of life for people living with HIV,” said Gary H. Gibbons, M.D., director of the National Heart, Lung, and Blood Institute. “Additional research can further expand on this effect, while providing a roadmap to rapidly translate research findings into clinical practice.”
For the double-blinded phase 3 trial, known as Randomized Trial to Prevent Vascular Events in HIV (REPRIEVE) study, researchers randomized participants into either a treatment group where they received a daily statin (pitavastatin calcium) or a control group where they received a placebo. The researchers followed participants for about five years, but ended the trial early when they discovered the treatment benefits outweighed the potential risks.
Researchers required those enrolled in the trial to have normal liver and kidney function. Participants were also required to take antiretroviral therapy, which was considered by the researchers to be critical to reducing the risk of HIV complications and related illnesses, including cardiovascular disease.
September 20, 2023
NIH Launches HIV Vaccine Trial in U.S. and Africa
A trial of a new HIV vaccine, supported by the National Institutes of Health, begins enrollment at six sites in the U.S. and South Africa.
Learn More.
The research study will determine whether a novel vaccine known as VIR-1388 is safe and able to to induce an HIV-specific immune response in people, according to the NIH.
VIR-1388 is designed to instruct the immune system to produce T cells that can recognize HIV and signal an immune response to prevent the virus from establishing chronic infection, according to Carl Dieffenbach, Ph.D., Director of NIH’s Division of AIDS.
In a NIH media advisory, Dr. Dieffenbach explained that VIR-1388 uses a cytomegalovirus (CMV) vector to deliver the HIV vaccine material to the immune system without causing disease in the study participants.
“CMV remains detectable in the body for life, which suggests it has the potential to deliver and then safely help the body retain HIV vaccine material for a long period, potentially overcoming the waning immunity observed with more short-lived vaccine vectors,” Dr. Dieffenbach said.
October 2, 2023
CDC Updates Doxy-PEP Guidelines for STI Prevention
The Centers for Disease Control and Prevention drafts guidelines on using Doxy-PEP to prevent some bacterial sexually transmitted infections (STIs)
Learn More.
STIs can increase a person’s risk of getting or transmitting HIV, and the number of STI cases in the U.S. rapidly increased in the early 2020s, according to the CDC. Doxy-PEP has demonstrated substantial benefit in reducing new chlamydia, gonorrhea, and syphilis infections, Dr. Leandro Mena, Director of the CDC’s Division of STD Prevention, stated.
The CDC’s draft guidelines provided an overview of monitoring for antibiotic use and antibiotic resistance that the agency will be considering to address potential risks. An informational presentation about the draft guidelines is available online.
The 2021 CDC STI Treatment Guidelines included a systematic review of the available literature on STI PEP and concluded that further studies were necessary to determine whether it would be an effective strategy for bacterial STI prevention. Since that time, promising results from several randomized trials on STI PEP indicated the need to re-address this topic. The new guidelines will offer an important resource for healthcare providers to inform the use of Doxy-PEP for preventing bacterial STI infections.
October 3, 2023
Future Success of PEPFAR Jeopardized by Anti-Abortion Agenda
After 20 years of receiving bipartisan funding support in Congress, PEPFAR (President’s Emergency Plan for AIDS Relief) is in danger of being dismantled due to anti-abortion extremists in the U.S. House of Representatives.
Learn More.
In the two decades since its launch by then-President George W. Bush, PEPFAR has saved an estimated 25 million lives around the world and has been reauthorized by the Congress every five years. However, in the fall of 2023, the Republican-majority Congress added abortion bans to the PEPFAR reauthorization bill and restricted the funding to one year. This has caused the legislation to stall in the Senate, according to the non-partisan Center For American Progress.
“Now, what should be another routine five-year reauthorization of PEPFAR has become an anti-abortion soapbox: A small group of extreme right-wing members of Congress are holding captive PEPFAR’s reauthorization — and the welfare of millions of adults and children in Africa and other parts of the world—to advance a radical anti-abortion agenda,” said Sarnata Reynolds, a senior director at the Center for American Progress, an independent, nonpartisan policy institute dedicated to improving the lives of Americans.
When then-President George W. Bush announced PEPFAR in 2003, less than 50,000 people living with HIV in sub-Saharan Africa had access to antiretroviral therapy. Today, PEPFAR operates in more than 50 countries, according to the U.S. National Institutes of Health.
The Republican-led strategy to link the PEPFAR reauthorization to abortion bans began earlier in the year, when PEPFAR was in the news for its 20th anniversary of saving lives worldwide. The plan was put forth by “a coalition of right-wing, religio-political organizations, then by a think tank influential in extreme MAGA Republican circles, and finally by the leading House Republican anti-abortion crusader, Congressman Chris Smith (R-NJ),” according to Population Action International (PAI), a non-profit organization that uses research and advocacy to improve global access to family planning and reproductive health care.
“The organized campaign featured a flurry of letters, press releases and a deeply flawed report purporting to expose the Biden administration’s misuse of PEPFAR to ‘promote its domestic radical social agenda overseas’ and calling for a complete overhaul and restructuring of the program,” PAI stated in its 2023 World AIDS Day “Washington Memo.”
A U.S. State Department official told Time magazine that non-reauthorization will “limit PEPFAR’s ability to conduct longer-term procurement of critical commodities, reducing our ability to ensure the lowest possible prices and will hinder our ability to support timely scale-up of new product innovations, all of which would risk the lives of the clients that PEPFAR supports.”
Many global health practitioners and advocates have expressed concern that even if PEPFAR is eventually reauthorized, the uncertainty of future funding created by Congress could ultimately increase program costs and inefficiencies as well as harm the U.S.’s diplomatic interests.
“Our appeal to the U.S. Congress is to reauthorize PEPFAR in order to sustain the gains we have achieved,” said Ummy Ally Mwalimu, Minister of Health of Tanzania, at a United Nations roundtable discussion.
October 18, 2023
CDC: PrEP Coverage on the Rise in U.S.
For the first time, more than one-third of people in the U.S. who could benefit from PrEP has been prescribed it, according to a new report by the Centers for Disease Control and Prevention.
Learn More.
Preliminary data published by the CDC publishes shows that in 2022, PrEP coverage is on the rise among Americans most likely to benefit from it. PrEP (pre-exposure prophylaxis) is highly effective for preventing HIV when taken as prescribed.
PrEP is available as a pill (Truvada® and Descovy®) or shots (Apretude). According to the CDC, people who can most benefit from PrEP meet any of the following conditions:
have had anal or vaginal sex in the past six months; and
have a sexual partner with HIV (especially if the partner has an unknown or detectable viral load),
have not consistently used a condom, or
have been diagnosed with a sexually transmitted disease in the past six months.
Or, have injected drugs, and have an injection partner with HIV or share needles, syringes, or other drug injection equipment (for example, cookers).
_ _ _ _ _
Source:
Centers for Disease Control and Prevention. Core indicators for monitoring the Ending the HIV Epidemic initiative (preliminary data): National HIV Surveillance System data reported through June 2023; and preexposure prophylaxis (PrEP) data reported through March 2023. HIV Surveillance Data Tables 2023;4(3). https://www.cdc.gov/hiv/library/reports/surveillance-data-tables/. Published October 2023. Accessed February 21, 2024.
December 2, 2023
2023 HIV/AIDS Report Indicates Progress Toward Goals in U.S.
The Biden White House releases the National HIV/AIDS Strategy 2023 Interim Action Report, signaling progress toward goals to end the HIV epidemic in the U.S.
The report shows that thanks to the efforts of community, state, and federal partners, our nation is making important progress toward the Strategy’s goals.
“This NHAS Interim Action Report does not declare victory, but serves as an ongoing call to action, highlighting the good work done by federal and community partners to energize and invigorate our collective national work to end the HIV epidemic and to ensure that no population or region is left behind,” wrote Harold J. Phillips, Director of Office of National AIDS Policy, in the Foreword of the report.
In a post for POZ magazine, Phillips urged stakeholders to recommit to taking necessary steps “to achieve our ultimate goal of ending the HIV epidemic in the United States.”
Since 2019, federal agencies and local communities have taken action as part of the Ending the HIV Epidemic initiative. The EHE initiative aims to scale up prevention and treatment strategies to reduce new HIV cases by 75% by 2025 and 90% before 2030 for an estimated 250,000 total HIV diagnoses averted.
Dr. Gao Yaojie, a medical worker who raised awareness about HIV/AIDS in rural China in the 1990s and early 2000s as government forces tried to restrict her actions, dies in exile in New York City. She was 95.
Learn More.
In the mid-1990s, retired gynecologist Dr. Gao Yaojie was providing medical care in a small village in rural China when one of her patients, a woman who was exhibiting advanced AIDS symptoms, tested positive for HIV.
Chinese officials had long held that HIV and AIDS was not a problem, because the country banned the importation of blood products. So Dr. Gao reached out to someone who might give her the hard truth about AIDS in China, Dr. Wang Shuping, a researcher who was testing blood donations for hepatitis C and HIV. Dr. Wang had found HIV in the blood supply, but her warnings to local officials were dismissed.
Drs. Gao and Wang decided to team up and launch a campaign to educate rural residents about HIV and AIDS, and the dangers inherent in the for-profit blood centers that paid for their plasma donations.
While Dr. Wang worked behind the scenes gathering facts and information, Dr. Gao became the public face of AIDS awareness in China, daring to publicly challenge China’s health system and government. This proved to be a very dangerous endeavor.
Dr. Gao travelled to remote villages from her home in Zhengzhou, providing rudimentary medicine for fever, diarrhea and other symptoms of AIDS. According to The New York Times, her stops included a village school where 20 children were left without parents due to AIDS. She said she once came across a toddler who was clinging to the feet of his mother, who had hanged herself after her husband died of AIDS. Dr. Gao also spent considerable time leafleting bus stations, health clinics and sex parlors with educational material about HIV/AIDS.
While Dr. Gao’s work on AIDS education in rural China later earned her international acclaim from world leaders including Hillary Clinton, her rising profile meant she also came under close state surveillance. Chinese officials forbid her to grant interviews, but she would still find ways to share her experiences dispensing healthcare and information in rural China.
Her cohort Dr. Wang also found ways to continue their work. After party officials shut down her research clinic, Dr. Wang took on a new job in Beijing as assistant to the chair of China’s National Committee on HIV/AIDS. Her position allowed her to continue her medical research on the prevalence of HIV/AIDS in China and keep Dr. Gao up-to-date on the latest information to share with rural residents.
In April 1996, all the donation clinics in China were abruptly shut down, without any notice to donors that they had been exposed to HIV through the clinics’ unhygienic practices. Later that year, clinics reopened with HIV testing for previous donors. And still, Chinese leaders would not acknowledge the prevalence of HIV in the country’s blood supply or the existence of an AIDS crisis among its rural citizens.
In spite of this, word got out to the rest of the world that China was experiencing an AIDS crisis. The epidemic in China was unique in that it was associated with the “bloodheads,” the commercial blood donation sites that proliferated in China after its 1986 ban on the importation of blood products.
On August 8, 2001, Chinese officials finally acknowledged that the country had been unsuccessful in quarantining itself against HIV, and announced a publicity campaign to educate its citizens about HIV and AIDS. However, Chinese officials claimed that the major causes of HIV transmission in China were drug use and sexual contact. Drs. Gao and Wang disputed this, making the research-supported claim that the country’s blood products industry was to blame.
“I visited so many provinces, cities, and counties, and met with thousands of AIDS patients. But I never saw a drug user and found that sexually transmitted cases accounted for less than 10%,” Dr. Gao told Radio Free Asia. “There is a 100% certainty that transmission is occurring through blood transfusions.”
Disputing the government’s official position on the health crisis was dangerous. Under Communist Party rule, Dr. Gao was able to continue providing care to people living with HIV and AIDS in rural China, and she was able to write books about it. But government officials heavily edited her work and kept a close eye on her public presence.
Officials refused to issue Dr. Gao a passport in 2001 to travel to the U.S. to be honored by the Global Health Council with the “Jonathan Mann Award for Health and Human Rights.” In 2003, government officials would again refuse to allow Dr. Gao to travel abroad to accept the Ramon Magsaysay Award for Public Service, which was presented at an event in Manila, Philippines.
In 2007, the Vital Voices Global Partnership invited Dr. Gao to Washington, DC to receive the Global Women’s Leadership Award for Human Rights at a March event. On February 1, as Dr. Gao was leaving for Beijing to pick up her travel visa, she was intercepted by officers and placed under house arrest, according to The New York Times. Officials turned off her phone service and prevented family members and friends from visiting her. Under duress from a party official who came to her apartment three times a day, Dr. Gao agreed to decline the invitation.
Dr. Gao didn’t realize that her house arrest was receiving worldwide attention in the media and many were outraged at China’s treatment of the 80-year-old activist. Hillary Clinton, who was then the Senator from New York and a co-founder of the nonprofit women’s advocacy group Vital Voices, wrote a letter to then-President Hu Jintao, urging him to allow Dr. Gao to come to the U.S. to accept the honor that her organization wanted to bestow. A few days later, he relented under the pressure.
In early March 2007, Dr. Gao made her first trip to the U.S. and was honored in Washington, DC. At the Vital Voices Awards event, she expressed concern that when she returned to China, she would be targeted by government officials for criticizing their handling of the AIDS epidemic.
Later the same year, she received another honor, the Heinz R. Pagels Human Rights of Scientists Award from the New York Academy of Sciences.
In August 2009, at the age of 82, Dr. Gao fled China with the help of the Chinese rights watchdog China Aid Association, and received political asylum in the U.S. She settled in the Harlem neighborhood of New York City, where she restored her writings to their pre-censored state and arranged to have them published.
For many years, she was visited by Chinese students and others who were aware of her human rights achievements. In March 2019, Hillary Clinton — who called Dr. Gao “simply one of the bravest people I know” — came to the doctor’s Harlem apartment for a visit.
“We’ve met many times over the years, including my first trip to China as secretary of state,” Clinton posted on Facebook after visiting Dr. Gao in New York City.
Dr. Gao’s “end-of-life” statement included her wish to be cremated and her ashes to be scattered in China’s Yellow River with no ceremony. Originating in the Bayan Har Mountains in western China, the river flows through nine provinces of China and empties into the Bohai Sea in the east. The Yellow River basin is known as the birthplace of ancient Chinese civilization, earning the name as “the Mother River.”
“I want to float eastwards down the Yellow River, and basically disappear from this world,” she said.
February 22, 2024
Long-Acting HIV Treatment Shown to be Superior to Daily Treatment in Some Cases
A nationwide study shows that long-acting antiretroviral therapy (ART) is better at suppressing HIV replication for people unable to maintain viral suppression through an oral daily regimen, according to the National Institute of Allergy and Infectious Diseases (NIAID).
Learn More.
The study found that long-acting cabotegravir and rilpivirine administered every four weeks had superior efficacy to daily oral ART. Upon these findings, an independent Data and Safety Monitoring Board working with NIAID recommended halting randomization of the study participants and invited those on the daily treatment to switch to the long-acting ART. that all participants in the study should have the opportunity to choose long-acting ART to ensure the best possible health outcomes in the study.
The study, which was schedule to continue through February 2025, was sponsored by the NIAID in collaboration with the National Institute of Mental Health, the National Institute on Drug Abuse, ViiV Healthcare and ACTG, a global NIH-funded clinical trials network that designed and implemented the study.
About 70% of people with HIV in the United States who take oral ART achieve viral suppression, according to data from the Centers for Disease Control and Prevention. Viral suppression protects people with HIV from progressing to advanced disease and prevents HIV transmission to others. In 2021, the Food and Drug Administration approved cabotegravir and rilpivirine as an ART regimen for people with a consistent history of viral suppression. NIAID launched this study in 2019 to understand how this regimen would work in people with previous challenges taking daily oral ART as prescribed and who had not consistently maintained viral suppression.
The study was conducted across 31 sites in the United States including Puerto Rico. Participants were screened to ensure the HIV in their blood was not resistant to the study drugs and that they met other health and safety criteria. Once enrolled, they received comprehensive and incentivized adherence support while taking daily oral ART to achieve viral suppression.
ViiV Healthcare and Johnson & Johnson provided medications for this study.
February 29, 2024
New Statin Therapy Guidelines for PLWH Help Reduce Cardiovascular Disease
The Department of Health and Human Services releases new guidelines for the use of statin therapy in people with HIV, based on 2023 study results indicating that a daily statin reduced the risk of major cardiovascular events in people living with HIV by more than a third.
The new guidelines were based on the results of the NIH-supported Randomized Trial to Prevent Vascular Events in HIV (REPRIEVE) trial, a global study that demonstrated a daily statin medication reduces the increased risk of cardiovascular disease experienced by people living with HIV.
Steven Grinspoon, MD, professor of medicine at Harvard University and chief of the metabolism unit at Massachusetts General Hospital, led the REPRIEVE study. Dr. Grinspoon said that this research study, involving participants in 12 countries, found that the use of the statin pitavastatin calcium reduced the risk of major adverse cardiovascular events — including heart attack, stroke, and cardiovascular death — among people with HIV by 35%, according to HIV.gov. He added that the study found that the intervention was equally efficacious among men and women.
Simultaneous to their presentation at IAS 2023, the REPRIEVE study findings were published in the New England Journal of Medicine on July 24, 2023.
June 4, 2024
Doxy PEP Emerges as Effective Preventative for Sexually Transmitted Infection
Researchers release guidelines on doxycycline post-exposure prophylaxis (doxy PEP), urging clinicians to prescribe the treatment to prevent sexually transmitted infections in at-risk populations.
Learn More.
In its announcement of the guidelines, the Centers for Disease Control and Prevention hailed doxy PEP as the first new STI prevention tool in decades. According to the CDC, research on Doxy PEP found that it reduced the risk of getting a bacterial STI for gay, bisexual, and other men who are at increased risk for these infections (specifically, syphilis, chlamydia, and gonorrhea).
The CDC recommended clinicians to discuss doxy PEP with all gay, bisexual, and other men who have sex with men and transgender women with a history of at least one bacterial STI in the last 12 months. The recommended dosage and timing of the self-administered treatment was 200 mg of doxycycline within 72 hours of sex.
July 10, 2024
NIH Recommends Screening Procedure to Detect & Prevent Anal Cancer in PLWH
The National Institutes of Health (NIH) releases the first U.S. federal clinical recommendations to prevent anal cancer for people with HIV.
Learn More.
Among its guidelines, the NIH recommends that all adults with HIV be assessed at least once per year for anal abnormalities (such as pain, burning, or masses) and undergo digital anorectal examination. People under the age of 35 who are symptomatic or show signs of anal cancer during the examination should undergo standard anoscopy.
Anoscopy is a medical procedure that involves the examination of the anal canal and lower rectum using a small, rigid instrument called an anoscope. This procedure is typically simple, painless, and can be performed in a doctor’s office without the need for anesthesia. The procedure usually takes about 10-30 minutes to complete, according to the Cancer Treatment Centers of America.
Older people living with HIV who are symptomatic should undergo additional lab-based screening with a High Resolution Anoscopy (HRA), rather than standard anoscopy.
These guidelines were developed following the NIH-supported ANCHOR trial in 2022.
“ANCHOR data show for the first time that, like cervical cancer, anal cancer can be prevented even in high-risk populations, such as people living with HIV, who often have HSIL (high-grade squamous intraepithelial lesions) that can be difficult to treat,” said Joel Palefsky, M.D., of the University of California, San Francisco, who led the study.
Although anal cancer is relatively rare in the general population, it is the fourth most common cancer among people living with HIV, according to the NIH. The incidence of anal cancer is estimated to be 89 per 100,000 among men living with HIV who have sex with men and between 18.6 and 35.6 per 100,000 among women living with HIV. In comparison, the incidence of anal cancer in the general population is 1.6 per 100,000.
Nearly all cases of anal cancer are caused by infection of anal cells with cancer-causing types of human papillomavirus (HPV). If the immune system does not fight off the infection, the lingering infection can cause the cells to become progressively more abnormal, ultimately developing into HSIL and then, in some cases, into anal cancer.
The ANCHOR study is the first randomized controlled trial to determine whether treating anal HSIL is a safe and effective strategy for reducing the progression of HSIL to anal cancer.
In the phase 3 trial, which was carried out at 25 sites nationwide, 10,723 people age 35 or older living with HIV underwent screening for HSIL with high-resolution anoscopy. Of these, 4,459 people were diagnosed with HSIL. People in this group were then randomly assigned to receive treatment or to receive active monitoring with no treatment, the current standard of care. Most participants in the treatment group received office-based electrocautery, a procedure in which heat from an electric current is used to destroy abnormal tissue.
After a median follow-up of just over two years, 21 people in the active monitoring group were diagnosed with anal cancer, compared with nine people in the treatment group — a 57% reduction. The majority of the side effects in the treatment group were mild and included pain and bleeding.
“The data support treating anal HSIL as the standard of care for people living with HIV who are 35 years of age or older,” said Dr. Palefsky.
August 22, 2024
2022 Number of PWLH Receiving Care Increases by Nearly Double
The latest results from the Ending the HIV Epidemic in the U.S. (EHE) initiative show that EHE-funded providers served more than 22,000 clients new to care and 19,204 clients estimated to be re-engaged in care in 2022 — almost double the number compared to 2020.
Learn More.
In addition, the 2022 EHE data showed that by the end of the year, 79.2% of clients who were new to care and were receiving HIV treatment reached viral suppression, according to the U.S. Health Resources & Services Administration (HRSA). Viral suppression means they cannot sexually transmit HIV to their partner and can live longer and healthier lives.
demonstrating that in 2022, HAB EHE-funded providers served more than 22,000 clients new to care and 19,204 clients estimated to be re-engaged in care. This nearly doubled the number of new and re-engaged clients served by HAB EHE-funded providers in 2022 compared to 2020.
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
2027
2028
2029
1980s
1990s
2000s
2010s
2020s
In the year:
Lives lost to AIDS
New diagnoses of HIV
Back to top
Figures represent estimated lives lost in the year.
For the years 1982-1986, data is based on estimates from the Centers for Disease Control and Prevention (CDC), as reported in its Morbidity and Mortality Weekly Report. For the years 1987-2019, data is based on estimates from the National Center for Health Statistics (NCHS). Number of U.S. deaths attributed to HIV infection is in death certificate data (per the NCHS’s Tenth Revision of the ICD [ICD-10] for selecting underlying cause of death).
The first cases of what would become known as AIDS were discovered in Los Angeles in 1981. AIDS would soon become a global epidemic. Since 1981, over 700,000 lives have been lost in the US, and approximately 40 million globally. The World Health Organization recently estimated approximately 38 million people are living with HIV across the world.
Figures represent estimated new diagnoses for the year.
The Morbidity and Mortality Weekly Report (MMWR) series is prepared by the Centers for Disease Control and Prevention (CDC). For the period 1981-2007, the data for HIV diagnoses is based CDC estimates as reported in the MMWR.
For the period 2008-2019, the data for HIV diagnoses is from National HIV Surveillance System (NHSS).
HIV cases include persons with Stage 3 (AIDS) classification.
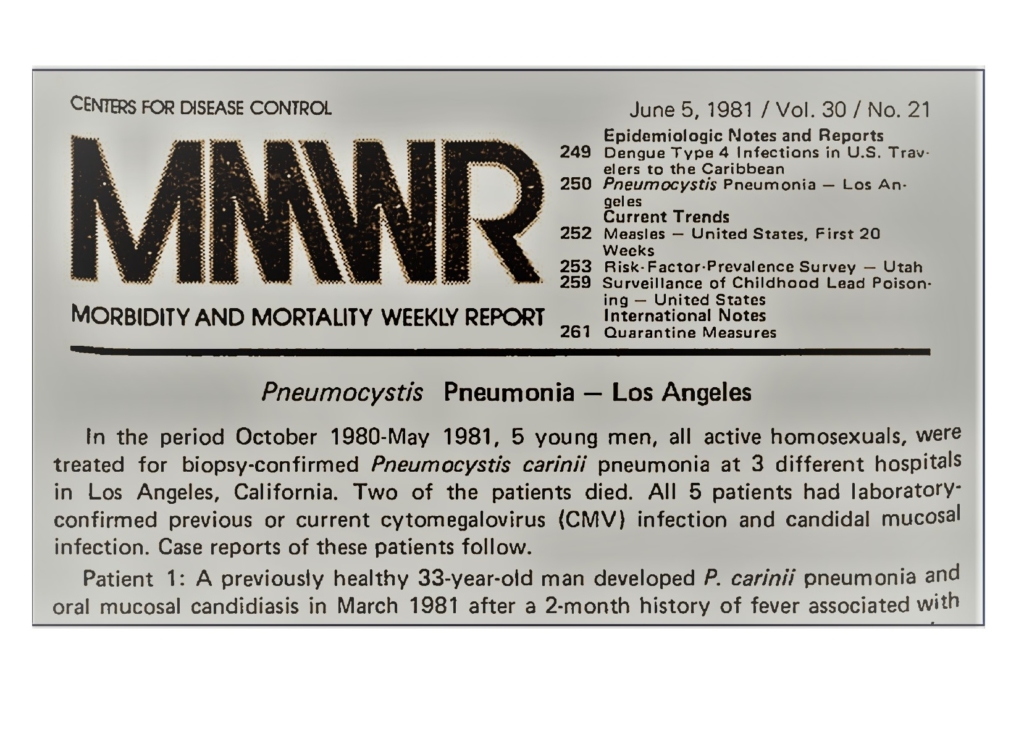


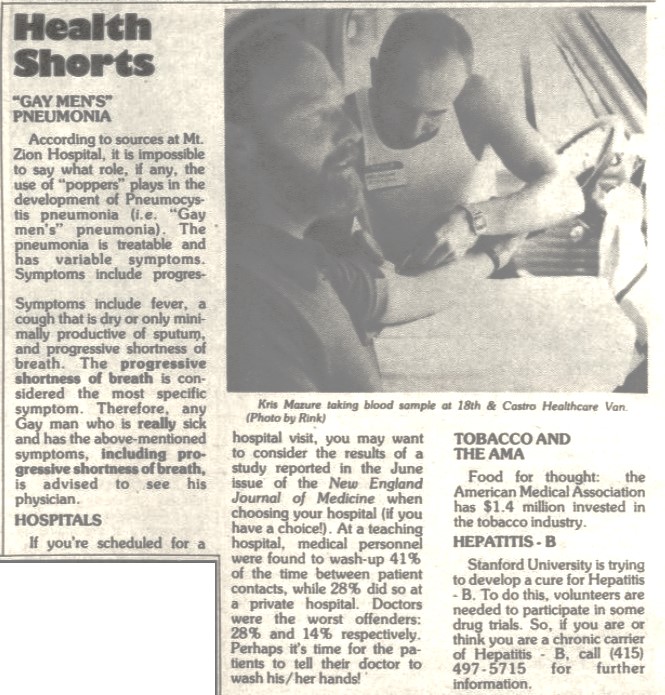

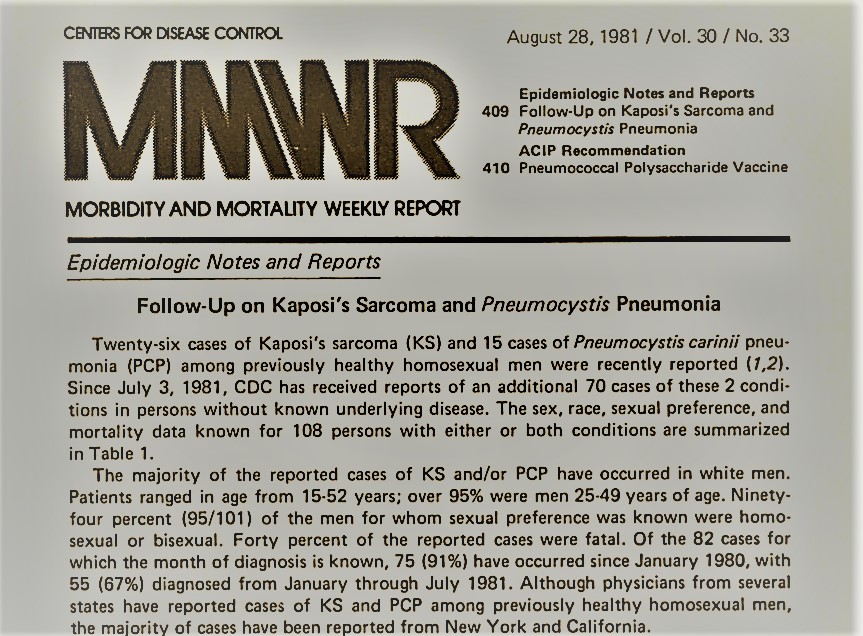


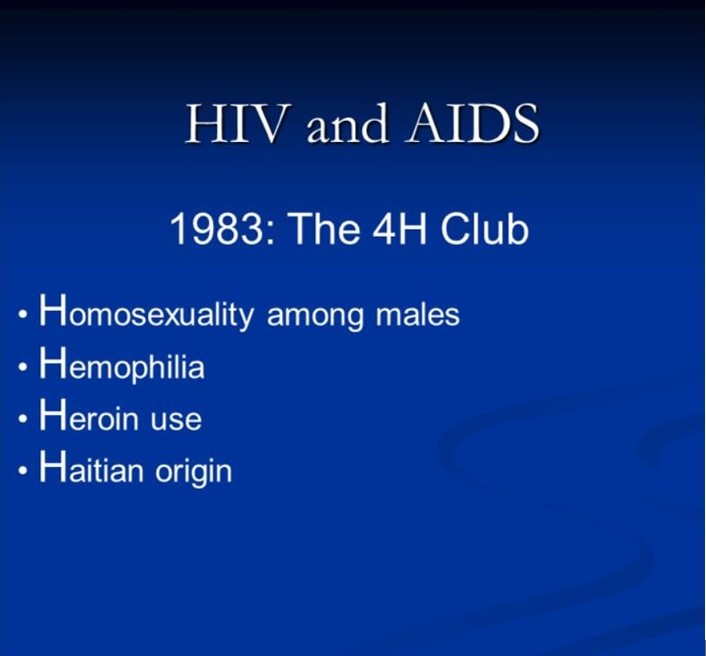
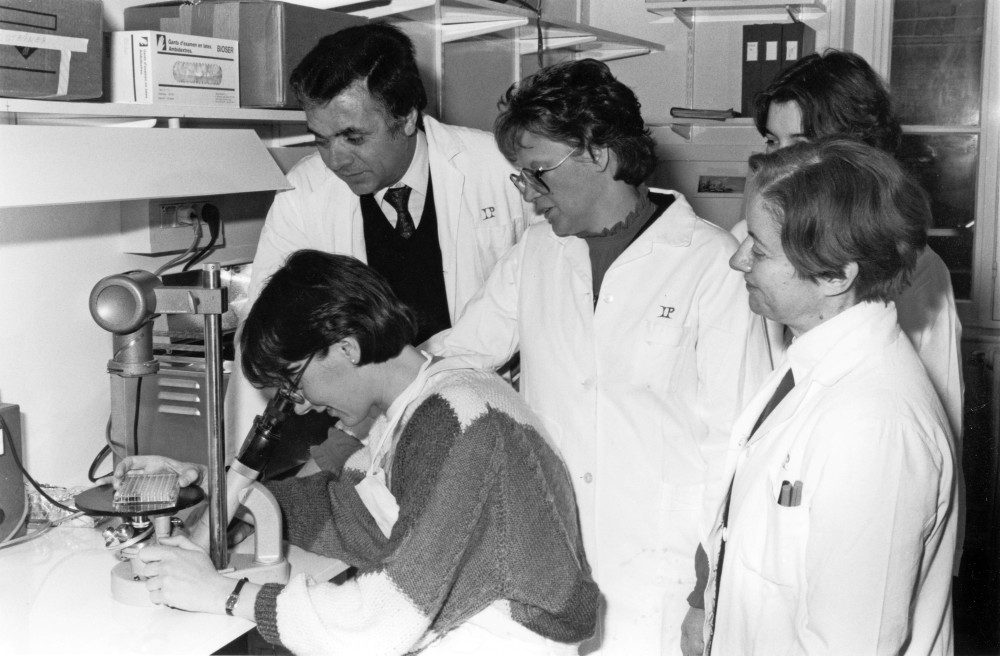

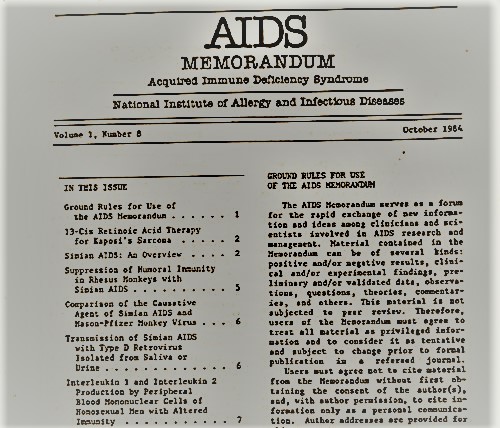
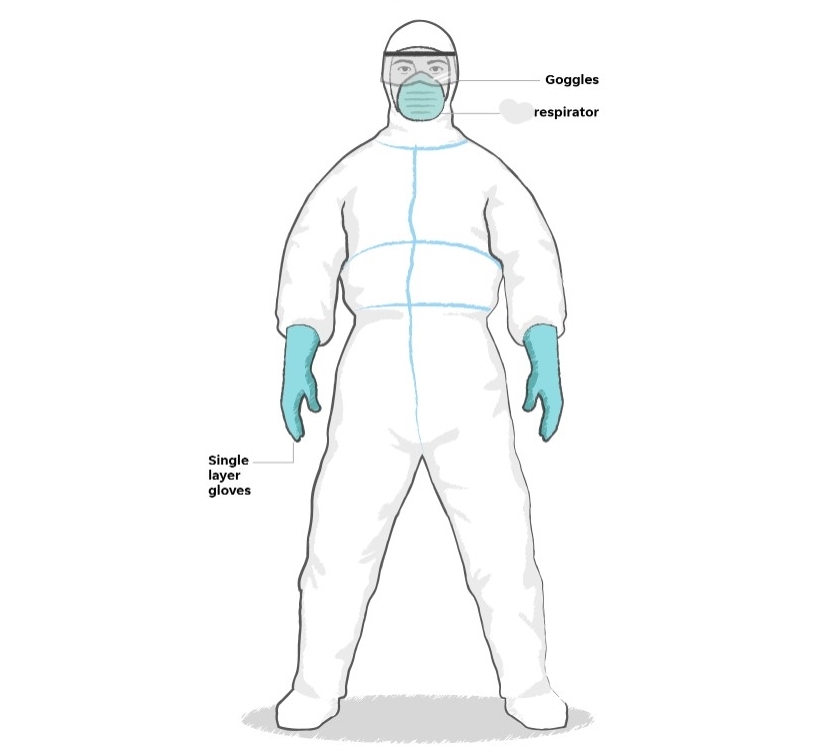


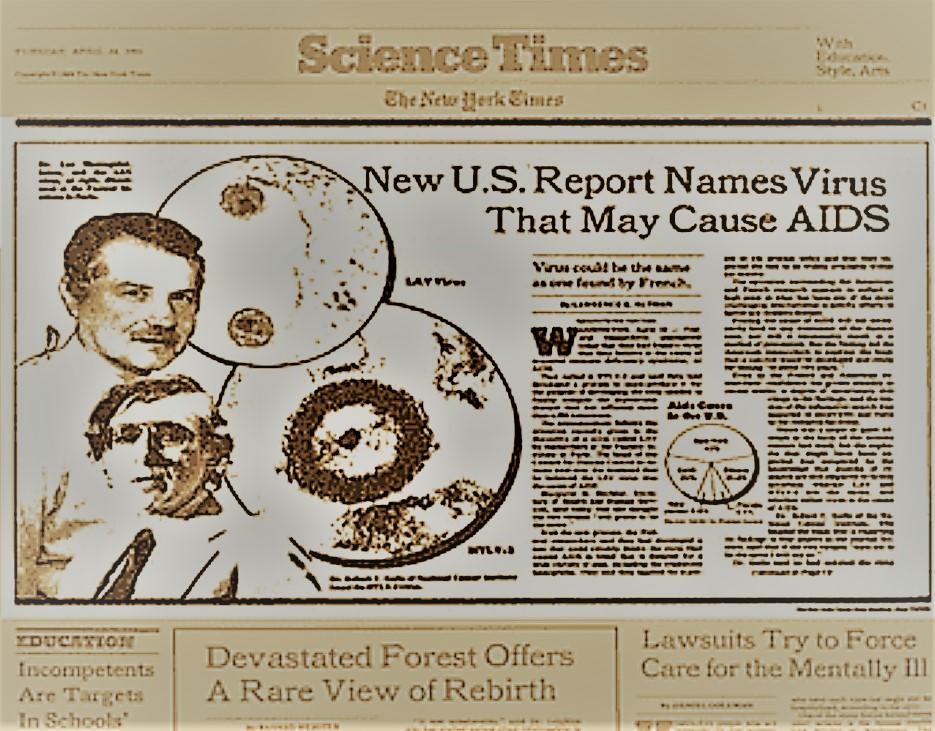

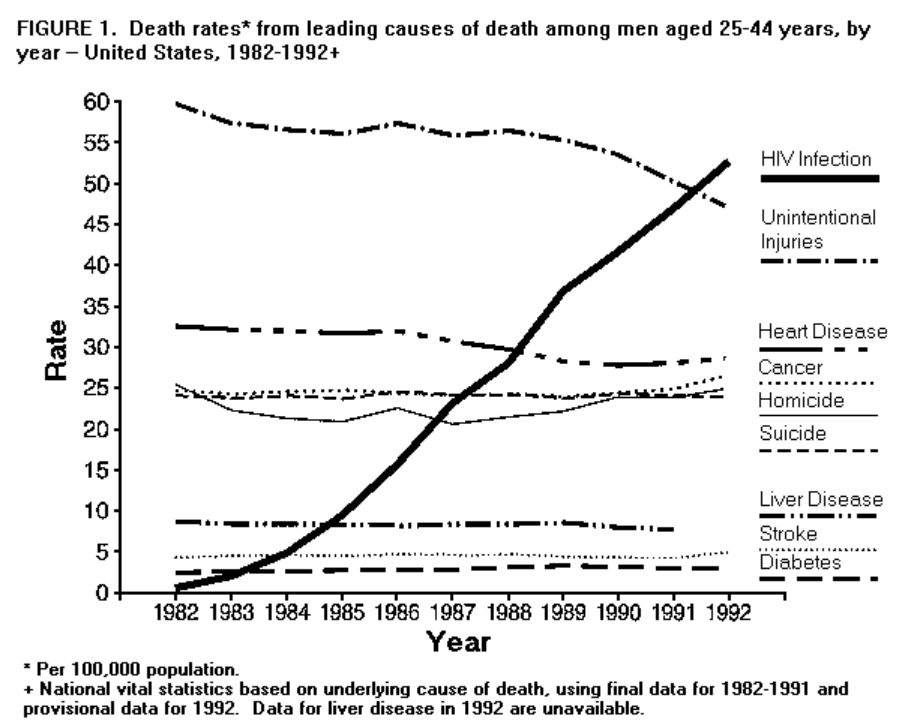

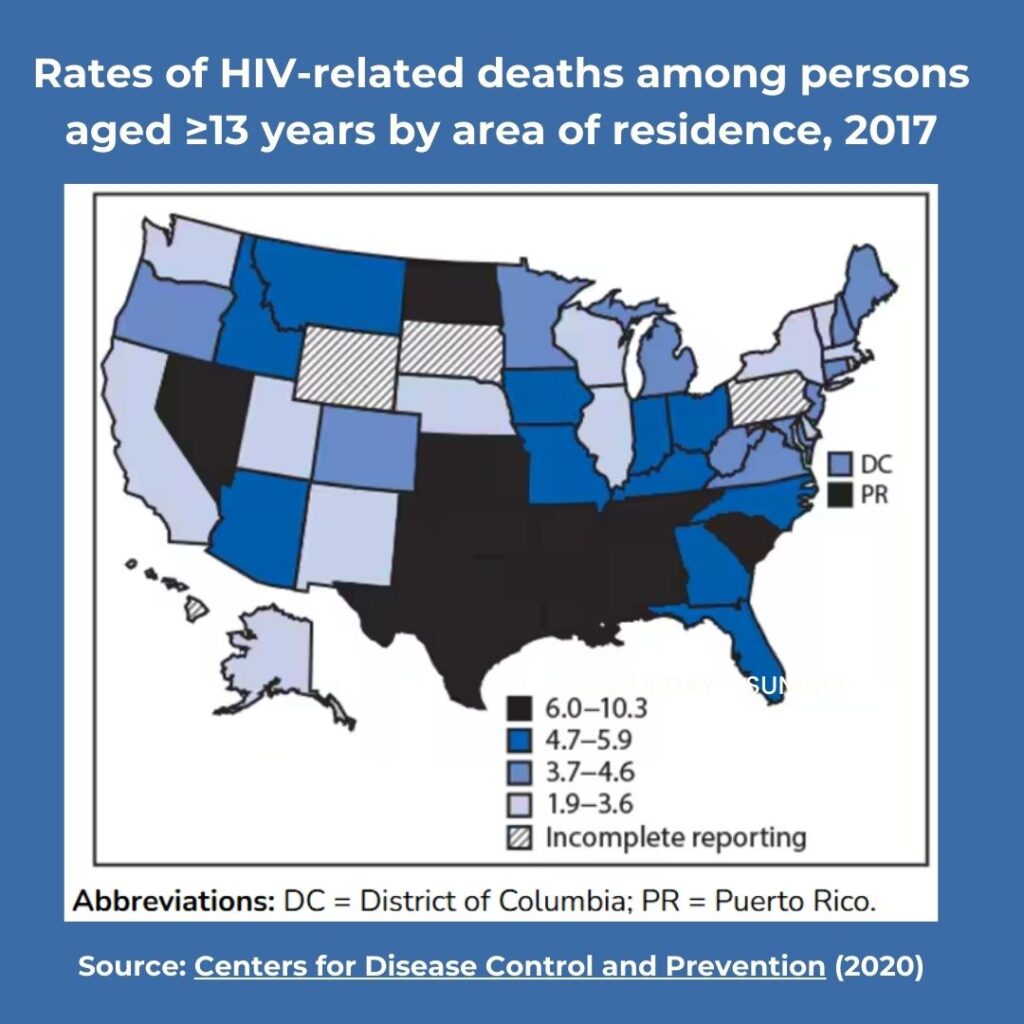



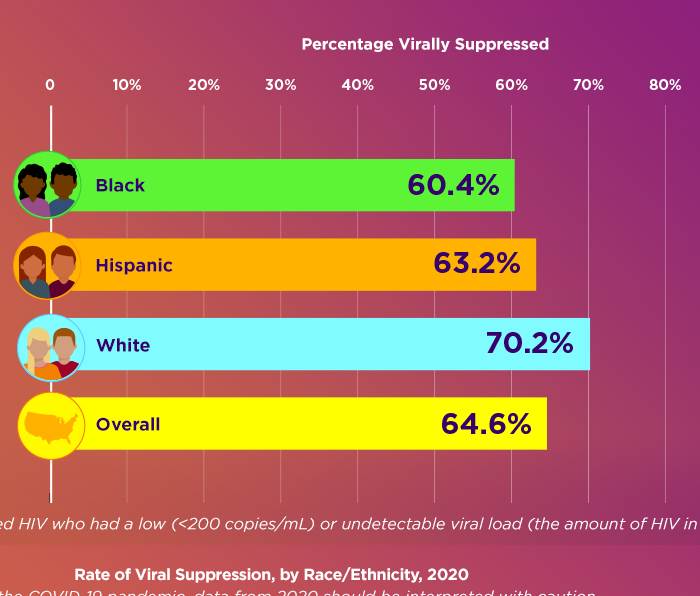
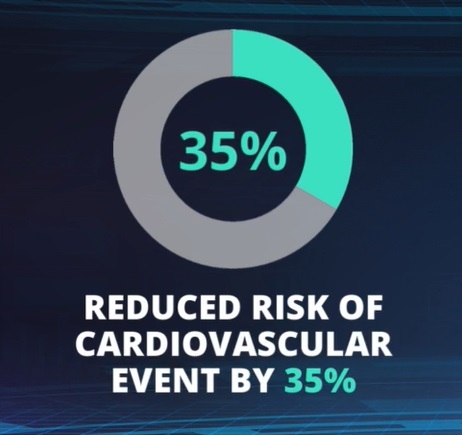



{kind=link}